Regular readers of my blog know that I tend to overthink things. Big time.
I’ve had a few days to think about what the radiation oncologist said in his email—about continued monitoring being a very reasonable approach—and I began to question that bit of advice. Not necessarily its validity, but more along the lines of why the change of heart with the doctor?
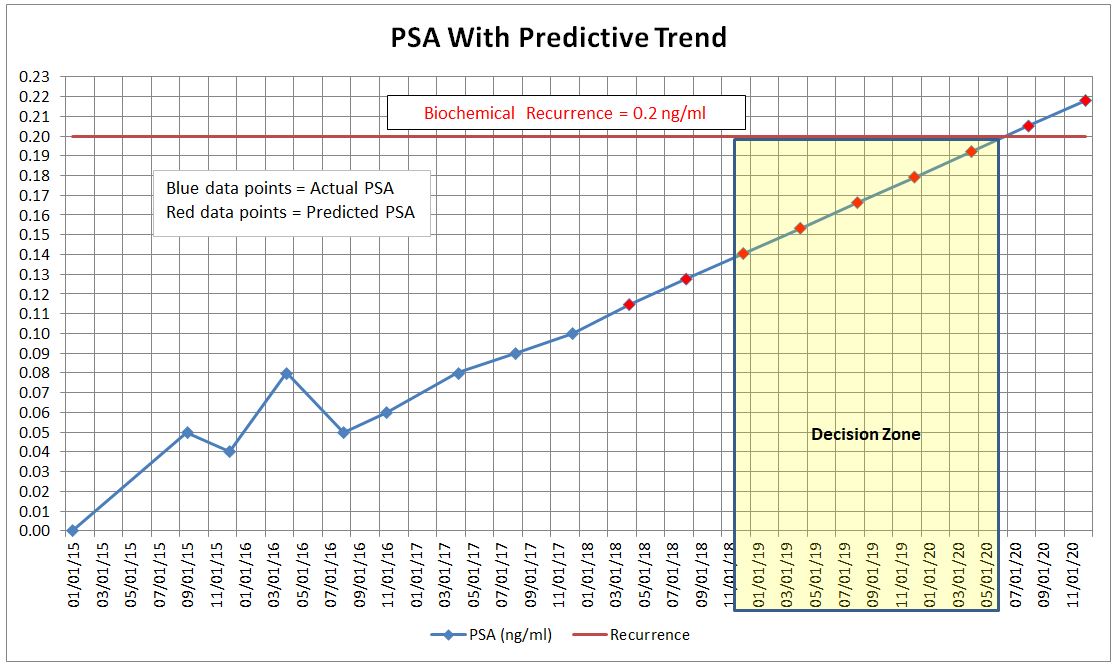
When we had our consult in May, there was no doubt that his recommendation was to start salvage radiation therapy right away. He presented a pretty strong argument that early treatment is better than delaying. My numbers now are the same as when he gave his “treat now” recommendation, so why the sudden change to “okay to monitor”? Is he just appeasing me, telling me what he thinks I want to hear? Or does this one data point of a stable PSA really justify changing a treatment recommendation?
Don’t fret. As I said, I overthink things.
I’m perfectly content with the “continue to monitor” approach for the foreseeable future. I really don’t question the integrity of the radiation oncologist either. Even if he was appeasing me, part of being a good doctor is listening to the patient’s concerns and understanding that the patient’s perspective needs to be at forefront of any treatment decision. I only met with the doctor once, but given his take-charge personality, I’m confident that he would have argued more forcefully if he truly thought I needed radiation therapy right away.
I’ve put aside my little bout of cynicism and will focus on enjoying the next four months.
Speaking of four months, that’s the other little cloud that rained on my post-PSA parade. “Crap. I’m back in PSA limbo land yet again.” Mentally, I had prepared myself for the PSA to have gone up again and that I would be one step closer to making the zap or not to zap decision. It’s still emotionally draining even after almost eight years of dealing with this. Oh well. Suck it up, buttercup.
On a fun note, I was toying with the idea of driving out to the 96° F / 36° C desert tonight to try and capture the Perseid meteor shower with my camera (I’m writing this on Friday night). But after three hours in the dentist’s chair this afternoon, that ain’t gonna happen. I’m zonked. Perhaps Saturday night.
Here’s what I captured after an hour and a half of standing alone in the desert last year. A near-full moon was rising and illuminating the mountains, but it was beginning to be too bright to see meteors.