Well, I missed last month’s post and this month’s is late. You would think that with all the quarantine time on my hands, I would have been a writing fool. Not so.
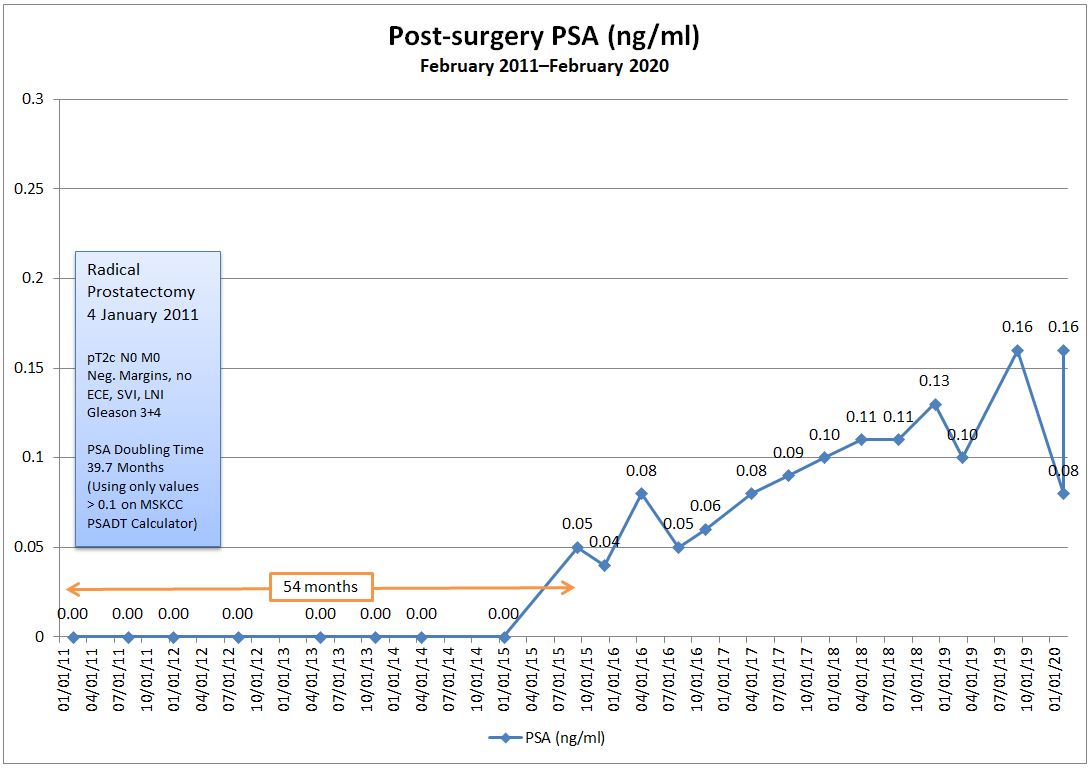
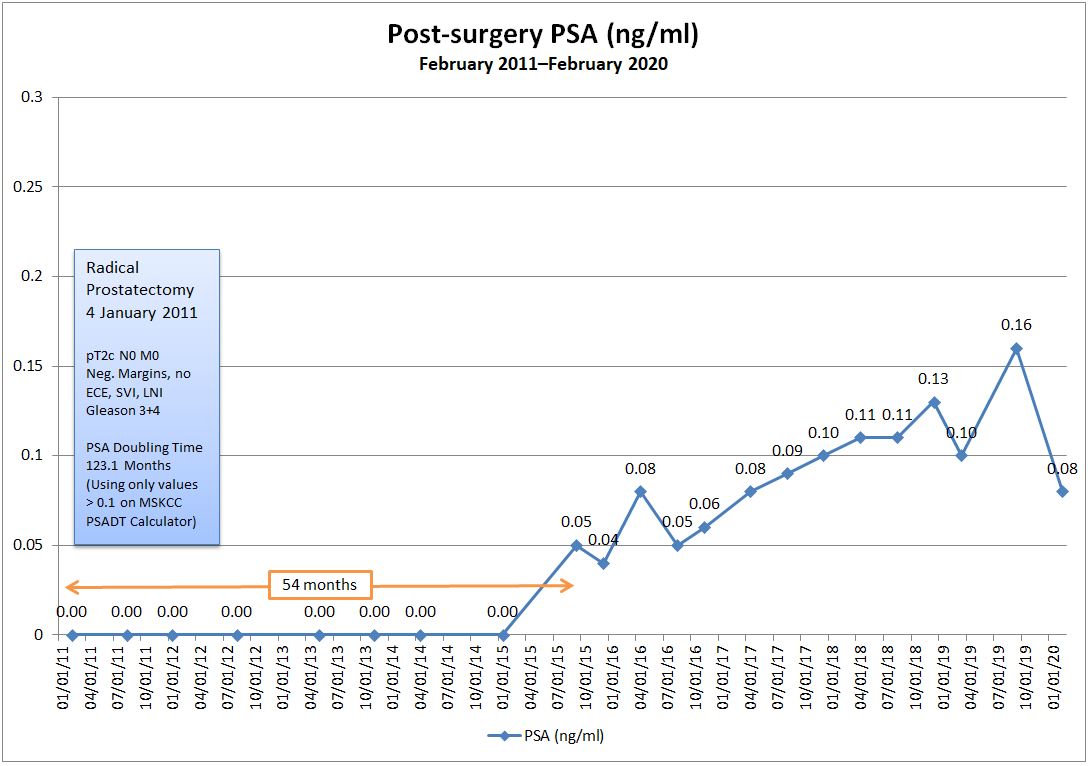
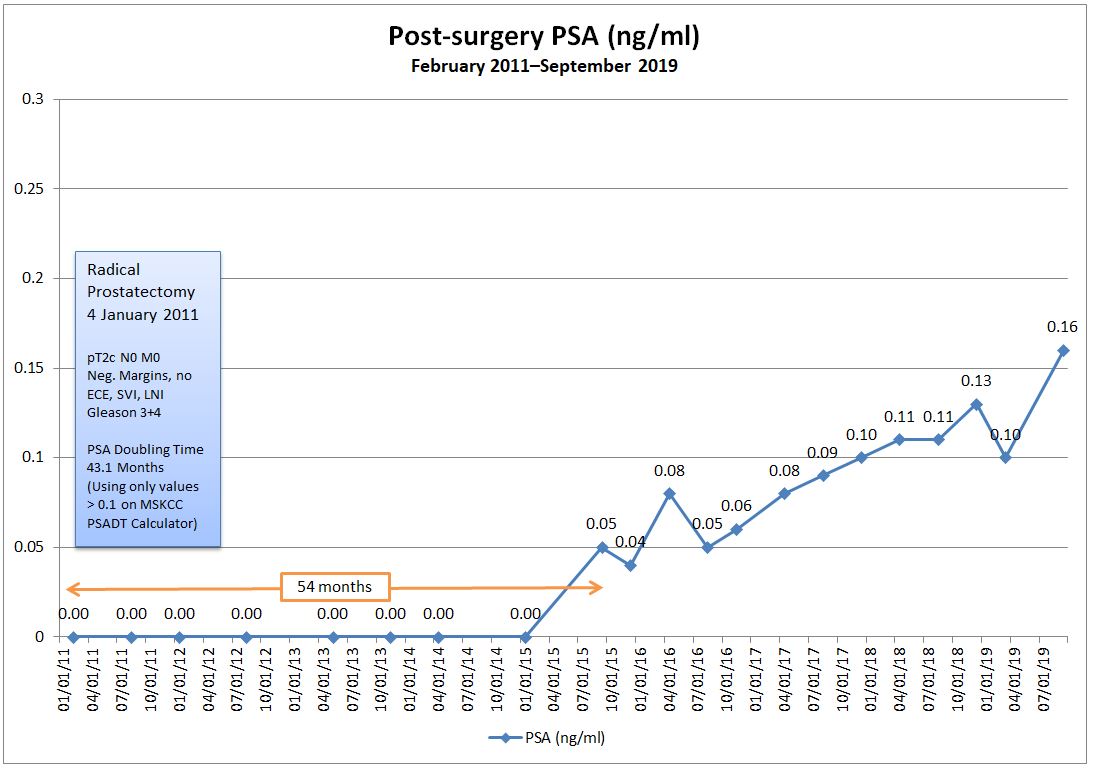
I did come across this study a while back that talks about PSA coming back after surgery and whether it’s wise to treat or watch.
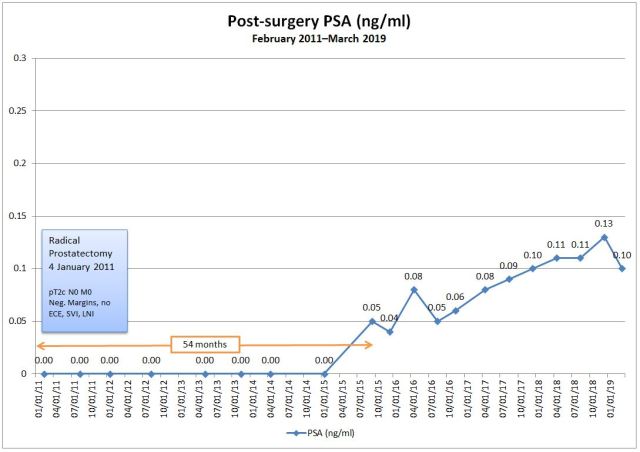
Low Detectable Prostate Specific Antigen after Radical Prostatectomy—Treat or Watch?
My interpretation of the paper with my specific numbers kind of reinforces what the doctor told me at my last visit: that I’m okay continuing to watch my PSA for now. Others with different numbers may come to a different conclusion. We’re all unique, after all.
I’m scheduled for my next follow-up with the doctor the first week of July, so I’ll have to get my blood drawn for the PSA test in late June, assuming the COVID restrictions are lifted by then.
You may recall my last post where I talked about taking medication to lessen the nerve pain in my leg. I started the medication on 30 March 2020 and I seemed to hit the side effects jackpot. They knocked me for a loop, at least initially (hence, no writing).
Headaches, dry mouth, nausea, diarrhea, and extreme fatigue plagued me the first two weeks, but the good news was that the nerve pain was reduced a good 50% to 70%. The side effects were so troubling in the first few weeks that, by the middle of the third week, I cut the dose in half, but the nerve pain returned.
I’m back on the full dose now, and my body seems to have adapted to a degree. The fatigue is still present, the dry mouth is still there, and the nausea is very mild and only early in the morning. (No, I’m not pregnant.) The pendulum swung in the complete opposite direction on my GI system–constipation is now the norm. Sorry. I’m oversharing once again.
We did discuss physical therapy as part of my treatment plan, but that was just as COVID was rearing its head, so that’s been put on hold for now.
I had been fortunate enough to be able to work from home since 16 March because of COVID-19, but I’ve returned to work in the office at the hospital beginning last week.
On the whole, I’m pretty comfortable being in the office again. Sure, there’s a more risk than just sitting at home, but my office is well away from a high-traffic area of the hospital and I’m literally the only person here. I don’t have to go into any of the wards, and the walk from my office to the exit is relatively short. I probably feel more at risk in the grocery store.
California was one of the first states to impose a stay-at-home order and we’re being very cautious and deliberate in our re-opening. Some will say that we’re being too slow, but not me. Our efforts really did make an impact on controlling the virus. We’ve got nearly 40 million people in the state and we have just over 80,000 positive cases and 3,240 deaths. Contrast that with New York state with 19.5 million residents with over 351,000 positive cases and 28,339 deaths.
No matter how you slice it, though, it’s universally tragic. We’re all anxious to get this under control and behind us.
Stay well!