My visits with the medical oncologists yesterday and today went well, and there was some consensus on how to proceed.
[BLUF: We’re kicking the can down the road three months.]
UCSD Oncologist
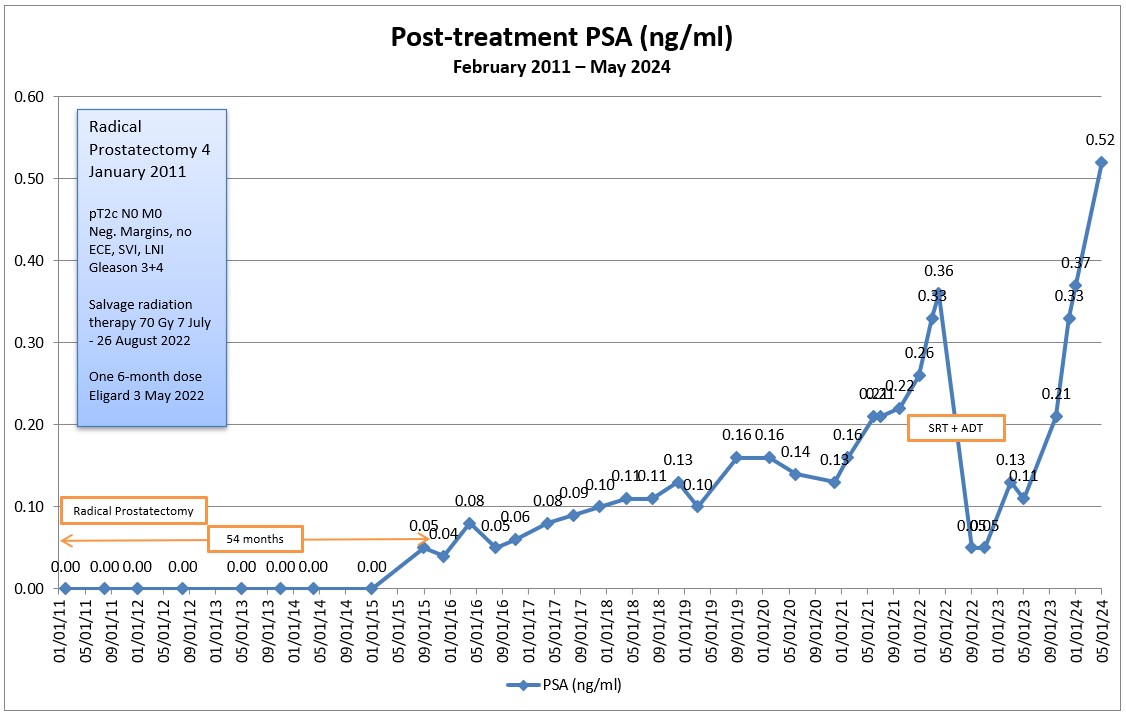
The first part of the meeting was getting the doctor up to speed on my case, as he didn’t have any of the history. Of course, nerd me came prepared with a two-page Reader’s Digest chronological summary of my diagnosis and treatment, printouts of my PSA charts, and copies of the PSA doubling time (PSA DT) calculations.
PSA Doubling Time
Because PSA DT is an important number in the decision-making process, I opened the conversation by asking him how many data points should be used in the calculations. He chuckled a bit before saying that one of the downfalls of using PSA DT is you can pick and choose the data that you want to get the answer that you want. So true.
I calculated my PSA DT using 3, 4, and 5 values and came up with different answers:
| Number of values used | Going back X months | Calculated PSA DT |
| 3 | 6 | 7.6 months |
| 4 | 9 | 8.0 months |
| 5 | 14 | 9.2 months |
He just looked at the curve on my PSA tracking chart and estimated in his head that it was around nine months. In his eyes, that six to nine month PSA DT warrants closer observation and monitoring.
Inconclusive PSMA PET scans
We discussed my four inconclusive PSMA PET scans and [F18] FDG PET scan, and whether he thought that I was PSMA negative. He thought it was unlikely that I was, offering up a case with another patient whose PSA was over 50 ng/mL and still showing up negative on PSMA PET scans.
One of the reasons that we talked about that at some length was that he suggested that Pluvicto / Lutetium-177 might be an option.
I asked about getting an Axumin scan or a Choline-11 scan, and he wasn’t in favor of doing either of those at the moment.
When to Start ADT
We also discussed when to start androgen deprivation (hormone) therapy (ADT). He didn’t have a set of specific criteria that he would use—e.g., specific PSA number, evidence of metastasis—but did focus in on the rate of PSA rise (PSA DT) and “patient motivations and preferences.”
What type of ADT
The doctor was a proponent of intermittent therapy in my case with six to twelve months on, then a similar period off. His goal would be to “maximize time off treatment” as long as my PSA is holding relatively steady and not going bonkers.
He seemed a tad hesitant to start with the combination therapy of ADT + ARPI (Eligard + Enzalutamide), but wasn’t opposed to it, either. He wasn’t a fan of trying the Enzalutamide alone because of its side effects (gynecomastia, in particular) and not seeing any substantial changes in long term outcomes.
Summary
I did share with the doctor the VA MO’s desire to start ADT + ARPI sooner rather than later, and he had a much lower sense of urgency in taking action. And, while I was a bonehead and didn’t explicitly ask him for his recommended course of action, the entire conversation led me to conclude that his preference was for continued close observation.
VA Oncologist
I technically didn’t meet with the oncologist; I met with a nurse practitioner who had reviewed my case with the oncologist just before (and during) my appointment.
Discussion
It was interesting that she opened the conversation with a quick review of my last appointment there, told me my PSA results from last week, and then said something along the lines of, “If you’re not ready to start ADT today, the doctor is okay with monitoring for another three months.”
At that point, I mentioned that I went to the UCSD MO the day before, and I spent a good chunk of time relaying how that meeting went.
I reminded her that I have the bone density scan in a few weeks and I intended to go through with that to establish a baseline even though we might not start ADT right away. She agreed.
I’m still meeting with the VA urologist on 23 June and want to get their thoughts on what’s next.
Summary
We’re going to do another PSA test in September, and the VA MO didn’t want to schedule an appointment with me until December with another PSA test just before that meeting, too. Interestingly, the VA MO also wanted to schedule a regular CT scan and bone scan ahead of the December appointment.
However, if the September PSA test jumps up significantly, we’ll revisit that plan based on the results. That may change doing the CT/Bone scans to another PSMA PET scan.
The Plan
In short, we’re going to kick the can down the road another three months.

More specifically:
- Bone density scan – 17 June
- Urologist appointment – 23 June
- PSA test – First week of September
- CT and Bone scan – First week of December
- PSA test – First week of December
- VA Oncology Appointment – 8 December
Summary
On the whole, I’m pleased with the plan as it stands right now. The UCSD MO emphasized the shared decision-making approach, adding in his notes, “Daniel is very well educated about his illness and understands there is no clearcut right and wrong answer.” Ain’t that the truth (about the no right or wrong answer).
Once I cleared the hurdles of getting set up in the UCSD system, I was impressed by the friendliness and professionalism of their staff in the department. They have a patient portal app that allows access to records and makes communicating about appointments—in both directions—quite easy.
One thing that I’ve noticed with both the VA and UCSD oncology departments is that their empathy and caring nature seems to be a notch or two above that of their respective urology departments. Not that the urology teams aren’t caring or empathetic; it’s just that the oncology folks seem to take it a step further.
I know the VA MO expressed a desire to take the lead on my case at my last appointment, and I’ll mention that to the urologist on the 23rd. And, for now, as pleasant as the experience at UCSD was, I plan on having the VA be my primary source of care.
More to come.
Be well!
Header image: Sunset, Imperial Beach, California