This interesting article appeared on my news feed.
https://news.cornell.edu/stories/2026/07/psa-levels-alone-may-not-reflect-prostate-cancer-growth


This interesting article appeared on my news feed.
https://news.cornell.edu/stories/2026/07/psa-levels-alone-may-not-reflect-prostate-cancer-growth

I’ve used the prostate cancer forums on the website HealthUnlocked to help gain other patient experiences as I move deeper into the world of advanced prostate cancer.
Recently, one of the forum moderators posted a link to this article:
The danger of doing your own research (or using AI)
It’s a rather blunt—perhaps even controversial—look at how patients research their diseases and treatments, but it does make you think about your own approach to becoming an educated patient and perhaps some of the pitfalls in doing so.
You may find it interesting. Or not.
Header Image: San Diego skyline from Coronado, California

One of my blog’s readers recently shared with me some information about the Prostate Cancer Promise research project (thanks, C.M.!).
It’s a project that’s seeking to collect DNA samples from patients at any stage of their prostate cancer so that they can identify certain patients with hereditary DNA mutations to track over the course of 15+ years in hopes of being able to help identify more tailored treatment options, as well as being able to let family members know that there is a gene that’s passed from generation to generation that makes them more prone to prostate cancer.
You will be selected for inclusion in the study if you have one of the hereditary mutations they’re looking for.
The research project is being conducted by Johns Hopkins University, the University of Washington, and Color, a company that specializes in DNA testing. The study is open only to U.S. citizens, and you can learn more about it either at their website, prostatecancerpromise.org, or their YouTube channel.
There’s a shorter cursory overview video followed by a more in-depth video below:
Disclaimer: I have no connection with the study, either as a participant or otherwise, and share this only for informational purposes only.
Header image: Grand Prismatic Spring, Yellowstone National Park, Wyoming
This showed up in my inbox and I found it interesting.
It appears to be focused on initial treatment rather than a salvage setting, and showed that even for those newly diagnosed with advanced prostate cancer that had already spread, there was benefit to radiating the prostate:
“The initial 2018 findings of this arm of the STAMPEDE trial were slightly surprising. Previous thinking was that if the cancer had spread then the horse had bolted and there was no point in shutting the stable door by treating the original disease site. These long-term results have confirmed that this is not the case, and by treating the original site after the disease has spread, some men with prostate cancer lived longer than those on hormonal therapy alone. This could potentially benefit people with other cancers that have spread to other parts of the body too.”
Professor Nick James, Professor of Prostate and Bladder Cancer Research at the ICR, and Chief Investigator of the STAMPEDE trial
Here is the link to the original article:
Long-term benefit of radiotherapy confirmed in advanced prostate cancer
A link to this article showed up in one of my prostate cancer newsletters that I receive. There’s a link to the original study report in the article, and it’s way over this layman’s head to make heads or tails of it in a brief read-through before my zapping session.
I didn’t dig deep enough to see if this applies equally to primary radiation therapy and salvage radiation therapy (because it’s not yet approved for use and too late for me).
A new study suggests that unwanted side effects of radiation treatments for prostate cancer could be reduced by the common steroid betamethasone.
Source: Common Steroid Could Improve Prostate Cancer Radiotherapy Outcomes

I came across this video highlighting Ga68 PSMA PET imaging from the doctor at the University of California San Francisco who helped with developing this imaging technique. It’s a bit long and a bit technical in some places, but gives a good overview.
Today was a tough day. The news of my PSA increasing to 0.21 ng/ml weighed heavily on me throughout the day. It even made me a little snippy in a meeting this morning, as my tolerance for trivial bullsh*t decreased to an all-time low. Oh well. They’ll get over it.
Long-time readers of this blog already know that I’ve delayed starting salvage radiation therapy because I’m reluctant to incur the short- and long-term side effects of radiation without having a higher degree of confidence that we’re actually zapping in the correct location(s)—zapping the cancer itself.
Of course, the current state of imaging for prostate cancer generally sucks, but it is getting better with advances like PSMA PET scans using 68Ga-PSMA-11 where prostate cancer can be located much earlier and much more accurately than using previous technologies such as bone scans. But even 68Ga PSMA PET scans have their limitations.
One of the greatest challenges (gambles?) in deciding when to start salvage radiation therapy is the timing. Most will argue the earlier, the better. Statistics show that in most cases, the cancer is still in the prostate bed or pelvic region, so the radiation oncologists start blindly zapping those regions hoping the statistics are correct. But the cancer could have already spread to more remote locations.
With my PSA doubling time in the 4-5 year range, my team and I have decided to hold off on salvage radiation therapy and, in so doing, I’ve avoided any radiation side effects for five years giving me a high quality of life during that time. That has value to me. Of course, none of us know whether the little buggers have been hanging out in the prostate bed during that time (like statistics would show), or if they’ve gone on one of their own infamous road trips and have started spreading.
One of the things that I’ve been trying to determine for months now is at what PSA level can the Ga68 PSMA PET scan begin to reliably pick up prostate cancer. The answer typically was in the 1.0 to 2.0 range for the PSA. With a PSA a fraction of that (0.21) the PSMA PET scan really wouldn’t be a reliable tool for me yet. It’s not a completely worthless tool, but there are decent chances that I could come away with a false negative result.
Tonight, I stumbled across this paper that provided some insights: Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial.
The chart below taken from the paper was exactly what I was looking for and more. First, it shows the number of cases where patients with an increasing PSA after prostatectomy have positive results based on their PSA level. For those with PSAs less than 0.5 ng/ml (me), the number of positive cases was only 38%. In other words, there’s about a one in three chance that the Ga68 PSMA PET will be able to locate the cancer at that PSA level. Not good odds, but better than zero.
To me, the really interesting thing about this chart is that it shows the location of where the PSMA PET scan found the cancer by PSA level.
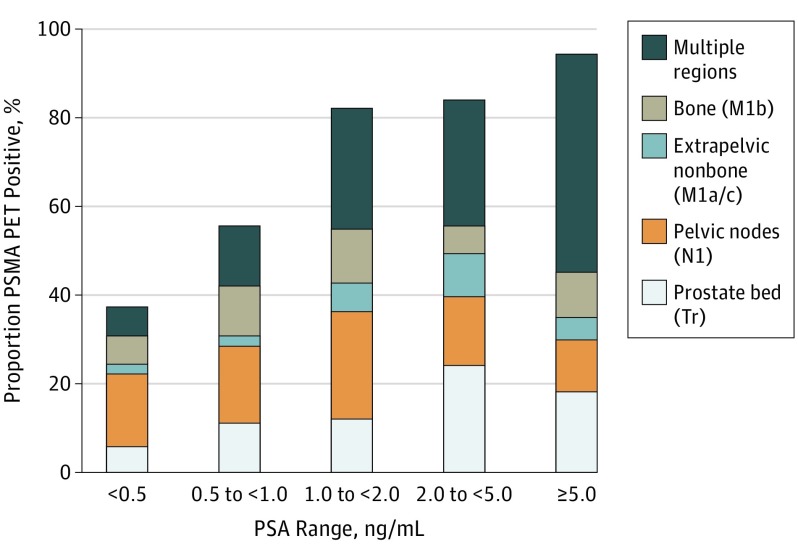
You can see that more than half of the cancer in patients with PSAs below 0.5 were found either in the prostate bed or pelvic region, both of which should be very treatable with salvage radiation therapy.
However, once the cancer is in other the other regions—extrapelvic nonbone (other organs), bone, or multiple regions—the cancer becomes very difficult if not impossible to treat. At that point, it’s only managed.
Please keep in mind that those are my non-expert opinions that I will have to confirm with my medical team to make sure I’m interpreting things correctly.
You can see that, as your PSA increases above 0.5 ng/ml, the cancer was found more broadly in the study participants. By that, I mean the cancer had spread beyond the prostate bed and pelvic region. You can also see, however, that even with PSAs less than 0.5, the cancer has already spread elsewhere in about 40% of the patients in the study with that PSA level.
That’s the whole point of knowing this. If the cancer has already spread, there’s no sense in zapping the prostate bed or pelvis risking long-term radiation side effects adversely impacting quality of life for no gain whatsoever.
This is only one study with 635 patients, so I am taking the results above with a healthy dose of skepticism, and I’ll continue to do more research in the three weeks before my appointment. But this study will be a good conversation opener for the consultation.
Some of the questions that are on the top of my bald head are:
Fortunately, the US Food and Drug Administration approved the Ga68 PSMA PET scan at the University of California Los Angeles (UCLA), and that would be a 2.5-3 hour drive for me to get up there to have the scan.
In the meantime, I’m going to have to reconcile in my own mind how high I’m going to let my PSA get before taking action, scan or not.
Lots of research, thinking, and soul-searching ahead. But be forewarned: My trivial B.S. tolerance level is way less than my PSA. 🙂
A recent report in the CDC’s Morbidity and Mortality Weekly Report (MMWR) may offer one of the best analyses of an increasing risk for diagnosis with and death from advanced forms of prostate cancer over the period from 2003 to 2017 (the last year for which we have accurate data from the SEER database). There […]
The epidemiology of prostate cancer (2003-2017) — THE “NEW” PROSTATE CANCER INFOLINK
Is it just me, or is anyone else having pandemic days all blend together and you lose track of time? Late last night (technically very early this morning as I was tossing and turning in bed around 2 a.m.), I realized, “Crap! I didn’t even think about posting on my blog, let alone write anything!”
So here I am on my advertised posting day with three hours and one minute left to get this out on the 11th, and I pretty much have nothing. Well, that’s not entirely true…
I did come across this article on The “New” Prostate Cancer Infolink that talks about PSA doubling times with respect to prostate cancer progression in men with non-metastatic castration resistant prostate cancer.
PSA doubling time and prognosis for men with nmCRPC
Unfortunately, they weren’t able to access the full study report, and the summary that’s provided is pretty high-level, restating the obvious: Shorter PSADT is associated with shorter metastasis-free survival and shorter overall survival.
One of the things that I discovered working in a hospital is that I can sometimes access research reports like this via its computer network. I’ll see if I can access this report to learn more details about the study and, if I can, I’ll share anything I learn.
Whew! Finished with time to spare. 🙂
Stay well and keep living the pandemic life as best and as safely you can wherever you happen to be.
Wow. I just may get this post out on time this month! I tell you, this pandemic thing has really thrown me for a loop when it comes to maintaining some sort of routine. Fortunately (or perhaps unfortunately), I’ve returned to working from the office every day for the last three weeks, and that’s brought some structure back to my life.
It’s hard to believe, but four months have passed since my last PSA test, and I’ll be heading off to the clinic on Tuesday morning. I hope. I haven’t actually confirmed that they’ve reopened for routine things like blood tests. If they are open and they do take the sample, I should have the results late Thursday night or Friday. My appointment to go over the results is on 2 July.
Just as a reminder, here’s my PSA roller coaster:
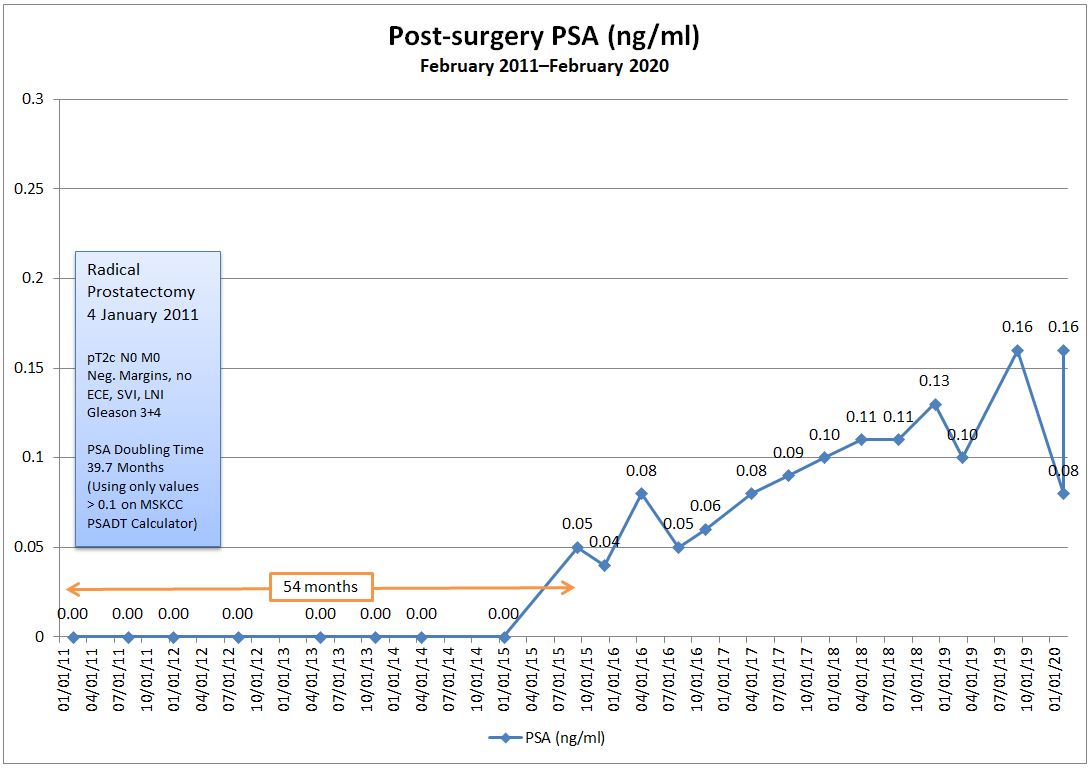
I’m at the point where I don’t get too worked up about these tests anymore, even with the upward trend. It is what it is and I’ll deal with the number when I get it.
The VA Greater Los Angeles Healthcare System is conducting a phase II trial “to determine whether a positron emission tomography (PET)/computed tomography (CT) scan using 18F-DCFPyL affects the clinical management plan in Veterans.” Some are saying that 18F-DCFPyL may prove to be even better than a Ga-68 scan.
For patients with biochemical recurrence, they want your PSA to be at least 0.2 in a post-radical prostatectomy situation, so unless my PSA jumps up again next week, I’m not eligible. (No, I’m not wanting it to jump up.) The cost is free to veterans and only veterans are eligible. You can learn more about the trial here:
18F-DCFPyL PET/CT Impact on Treatment Strategies for Patients With Prostate Cancer (PROSPYL)
So that’s about it from a toasty 90° F / 32° C San Diego.
Wear a mask. Stay apart. Stay well!
