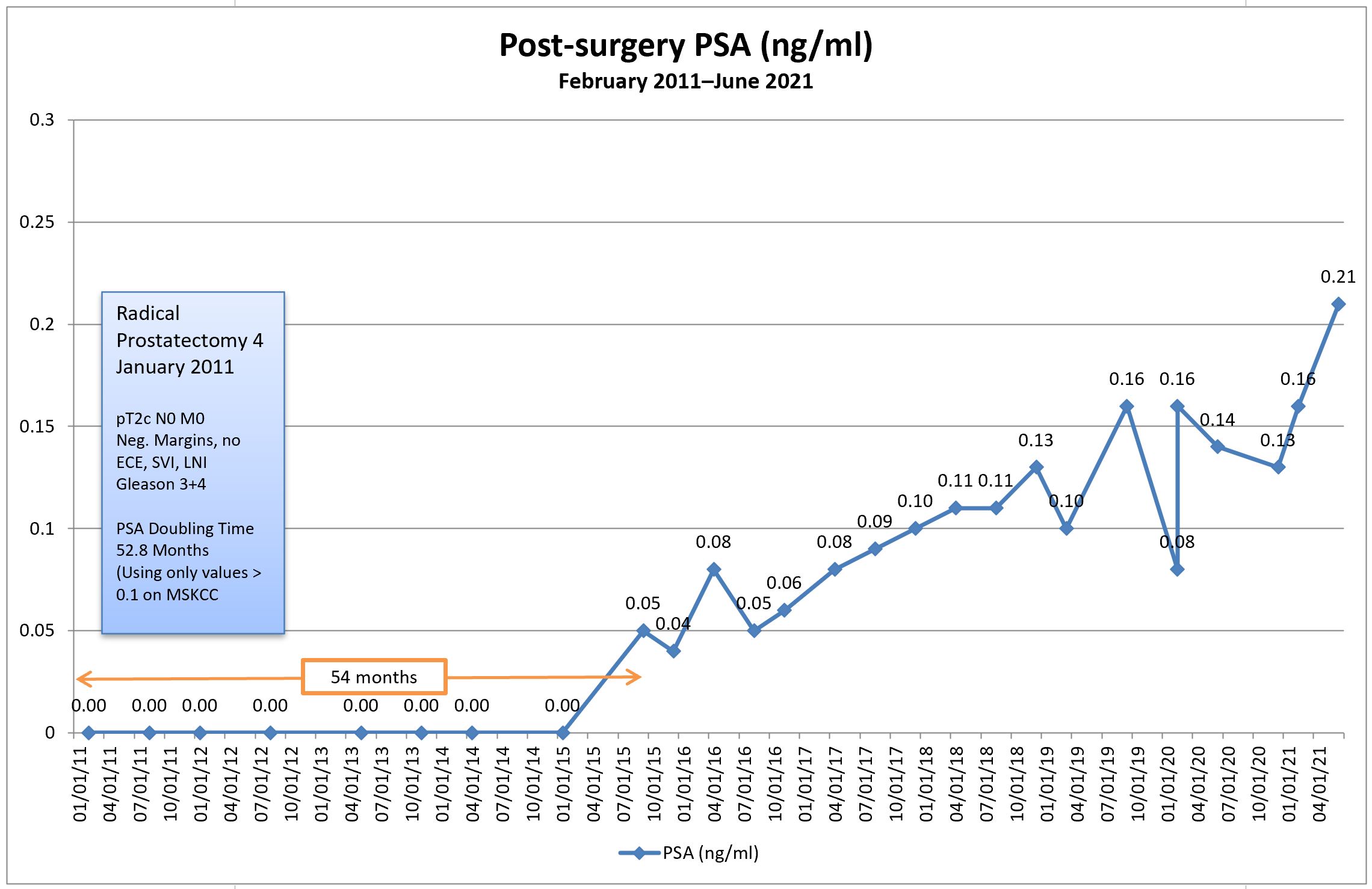
Today was a tough day. The news of my PSA increasing to 0.21 ng/ml weighed heavily on me throughout the day. It even made me a little snippy in a meeting this morning, as my tolerance for trivial bullsh*t decreased to an all-time low. Oh well. They’ll get over it.
Long-time readers of this blog already know that I’ve delayed starting salvage radiation therapy because I’m reluctant to incur the short- and long-term side effects of radiation without having a higher degree of confidence that we’re actually zapping in the correct location(s)—zapping the cancer itself.
Of course, the current state of imaging for prostate cancer generally sucks, but it is getting better with advances like PSMA PET scans using 68Ga-PSMA-11 where prostate cancer can be located much earlier and much more accurately than using previous technologies such as bone scans. But even 68Ga PSMA PET scans have their limitations.
One of the greatest challenges (gambles?) in deciding when to start salvage radiation therapy is the timing. Most will argue the earlier, the better. Statistics show that in most cases, the cancer is still in the prostate bed or pelvic region, so the radiation oncologists start blindly zapping those regions hoping the statistics are correct. But the cancer could have already spread to more remote locations.
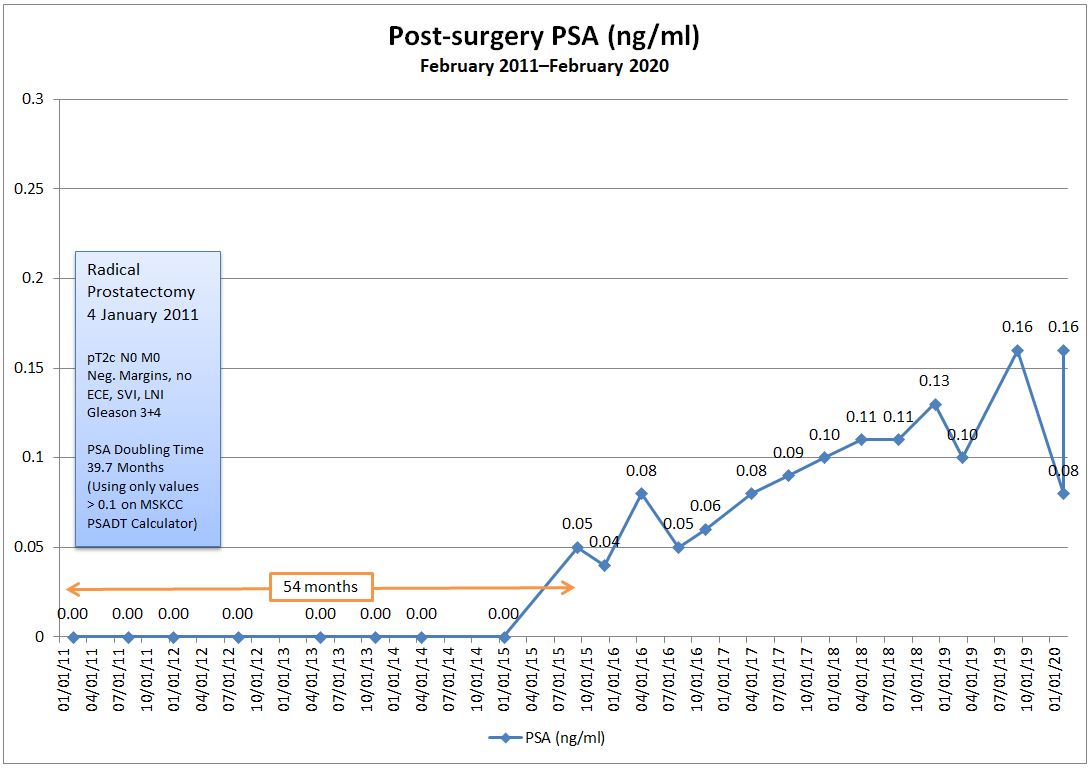
With my PSA doubling time in the 4-5 year range, my team and I have decided to hold off on salvage radiation therapy and, in so doing, I’ve avoided any radiation side effects for five years giving me a high quality of life during that time. That has value to me. Of course, none of us know whether the little buggers have been hanging out in the prostate bed during that time (like statistics would show), or if they’ve gone on one of their own infamous road trips and have started spreading.
One of the things that I’ve been trying to determine for months now is at what PSA level can the Ga68 PSMA PET scan begin to reliably pick up prostate cancer. The answer typically was in the 1.0 to 2.0 range for the PSA. With a PSA a fraction of that (0.21) the PSMA PET scan really wouldn’t be a reliable tool for me yet. It’s not a completely worthless tool, but there are decent chances that I could come away with a false negative result.
Tonight, I stumbled across this paper that provided some insights: Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial.
The chart below taken from the paper was exactly what I was looking for and more. First, it shows the number of cases where patients with an increasing PSA after prostatectomy have positive results based on their PSA level. For those with PSAs less than 0.5 ng/ml (me), the number of positive cases was only 38%. In other words, there’s about a one in three chance that the Ga68 PSMA PET will be able to locate the cancer at that PSA level. Not good odds, but better than zero.
To me, the really interesting thing about this chart is that it shows the location of where the PSMA PET scan found the cancer by PSA level.
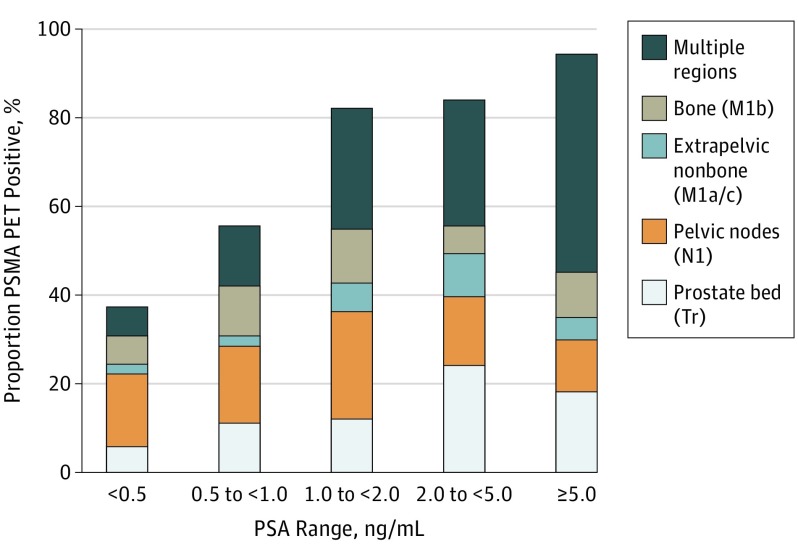
You can see that more than half of the cancer in patients with PSAs below 0.5 were found either in the prostate bed or pelvic region, both of which should be very treatable with salvage radiation therapy.
However, once the cancer is in other the other regions—extrapelvic nonbone (other organs), bone, or multiple regions—the cancer becomes very difficult if not impossible to treat. At that point, it’s only managed.
Please keep in mind that those are my non-expert opinions that I will have to confirm with my medical team to make sure I’m interpreting things correctly.
You can see that, as your PSA increases above 0.5 ng/ml, the cancer was found more broadly in the study participants. By that, I mean the cancer had spread beyond the prostate bed and pelvic region. You can also see, however, that even with PSAs less than 0.5, the cancer has already spread elsewhere in about 40% of the patients in the study with that PSA level.
That’s the whole point of knowing this. If the cancer has already spread, there’s no sense in zapping the prostate bed or pelvis risking long-term radiation side effects adversely impacting quality of life for no gain whatsoever.
This is only one study with 635 patients, so I am taking the results above with a healthy dose of skepticism, and I’ll continue to do more research in the three weeks before my appointment. But this study will be a good conversation opener for the consultation.
Some of the questions that are on the top of my bald head are:
- Should we run another PSA test to see if this was an outlier/anomaly like some of my previous PSA tests (I’ve been using the same lab all along)?
- How much weight does PSA doubling time have now that we’ve crossed the 0.2 ng/ml threshold?
- Would he support getting the Ga68 PSMA PET scan done at this PSA level?
- If not, at what PSA level would he support getting the PSMA PET scan?
- Would he be willing to give me a referral to get one done even if I have to pay for it myself?
Fortunately, the US Food and Drug Administration approved the Ga68 PSMA PET scan at the University of California Los Angeles (UCLA), and that would be a 2.5-3 hour drive for me to get up there to have the scan.
In the meantime, I’m going to have to reconcile in my own mind how high I’m going to let my PSA get before taking action, scan or not.
Lots of research, thinking, and soul-searching ahead. But be forewarned: My trivial B.S. tolerance level is way less than my PSA. 🙂