As a baby boomer, I grew up with Spock. Both of them.
First, there was Dr. Benjamin Spock, the noted pediatrician who told my parents—and millions of other parents—how to raise and care for their kids. Then, of course, there was the Star Trek Spock, whose existence was rooted in Vulcan logic.
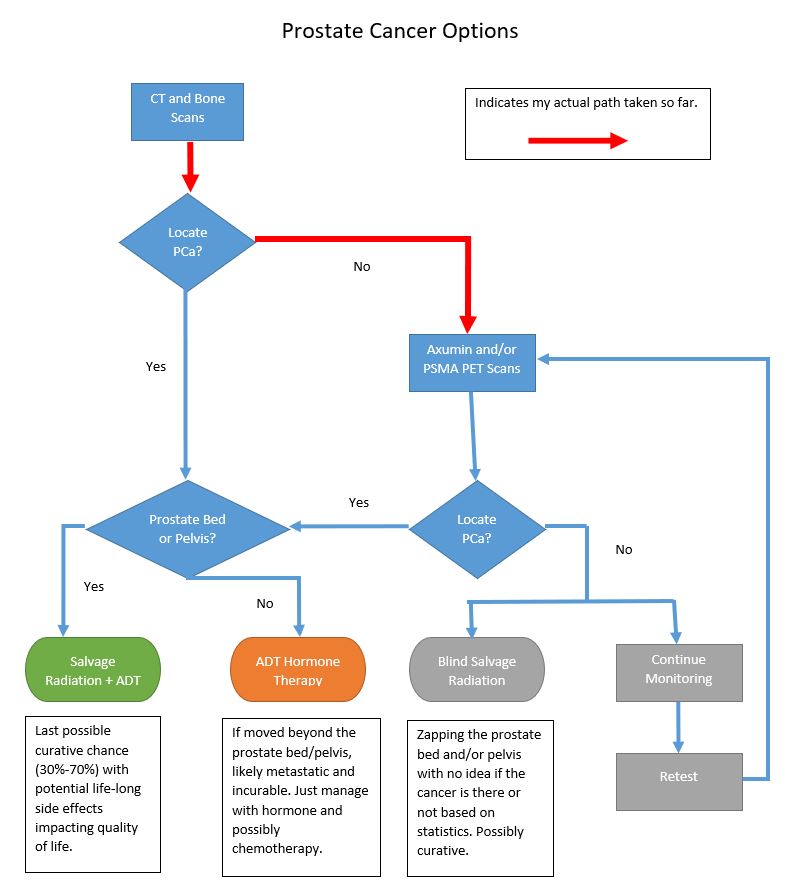
Now I’m not a Trekkie, but if you’ve read any part of this blog, you do know that facts, figures, and logic are high on my priority list, too. I thought, “What better way is there to outline the possible scenarios and decisions that are ahead of me than to put them all in a flow chart.” So here goes:
So let’s step through this.
We start with the CT and Bone scans that happened over the last two weeks. The first question is, “Did those scans determine the location of the prostate cancer (PCa)?”
If the answer is yes, then the next question is, “Was the prostate cancer in the prostate bed and/or pelvis?”
PCa in Prostate Bed/Pelvis
If the answer is yes, the PCa is in the prostate bed and/or pelvis, then Salvage Radiation Therapy (SRT) with or without Androgen Deprivation Therapy (ADT) (Hormone therapy) offers the last possible chance of a true cure. Of course, there are risks associated with SRT that would impact your daily quality of life: bowel control, bladder control, and lack of sexual function. Additionally, depending on which study you look at, SRT may be successful only 30% to 70% of the time. (Green bubble above.)
PCa is Not in Prostate Bed/Pelvis
But if the answer is no, the PCa is outside of the prostate bed and pelvis, that means the PCa is now distant and likely metastasized. If that’s the case, there is no cure and the PCa can only be managed with hormone therapy and perhaps chemotherapy. (Orange bubble above.)
CT and Bone Scans do not Locate the Prostate Cancer
We’ve talked at some length that neither the CT scan nor the bone scan have the sensitivity to pick up the cancer’s location based on my PSA level of 0.21 ng/mL. It was very likely that neither would pick up the cancer at that first decision point on the flow chart, so further investigation is required by using the Axumin or PSMA PET scan.
CT and Bone Scan Results
In fact, neither the CT nor the bone scan picked up the location of the cancer:
No definite scintigraphic evidence of metastatic bone disease and no evidence of a widespread osseous process
So that’s actually good news with the bone scan. It shows that it has not metastasized to the bones, which is definitely a good thing. (Or, at least if there is metastasis to the bones, it’s at a level that’s unable to be picked up by the sensitivity of the scan.)
Next Steps
We follow my red arrows above and run the Axumin or PSMA PET scans (or both) to see if either of those can pick up the location of the cancer. I’ll have that discussion with the urologist on 3 August 2021, and we’ll see when we can get them on the calendar.
If the Axumin and/or PSMA find the cancer in the prostate bed/pelvis, then we go back to the section above and land on SRT as the option. But if it’s found outside the prostate bed/pelvis, then we go back to the other section where we just manage with ADT. (If the lesion outside the pelvis is well-defined, it may be something that could be zapped in its location. Something to explore.)
If the Axumin or PSMA PET scan cannot locate the PCa, then things get fuzzy fast.
Sure, we could go ahead and blindly complete the salvage radiation therapy, hoping that we’re zapping in the correct place. Or, we could continue to monitor for a while longer and then retest to see if the cancer can be pinpointed.
This may have been a bit of an oversimplification of what’s ahead for me, but I’m hoping that it makes sense to you.
Be well!