The radiation oncologist threw a curveball that I wasn’t expecting at this morning’s appointment.
In a nutshell, he suggested doing concurrent androgen deprivation (hormone) therapy with the salvage radiation. That was not something that we discussed at our first meeting. The ADT would be for six months if done concurrently.
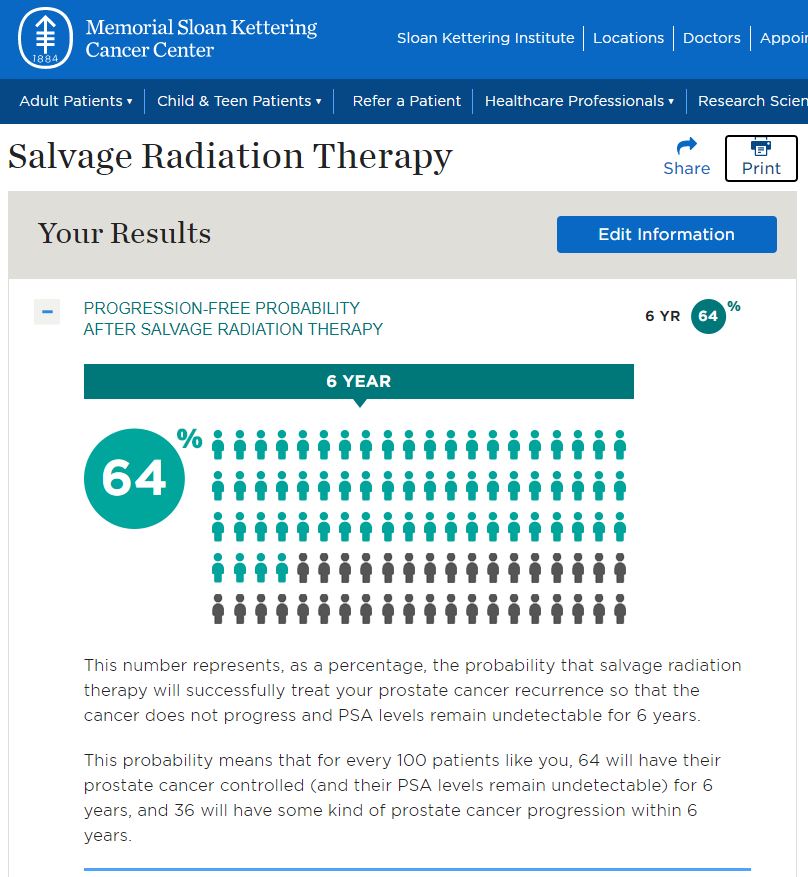
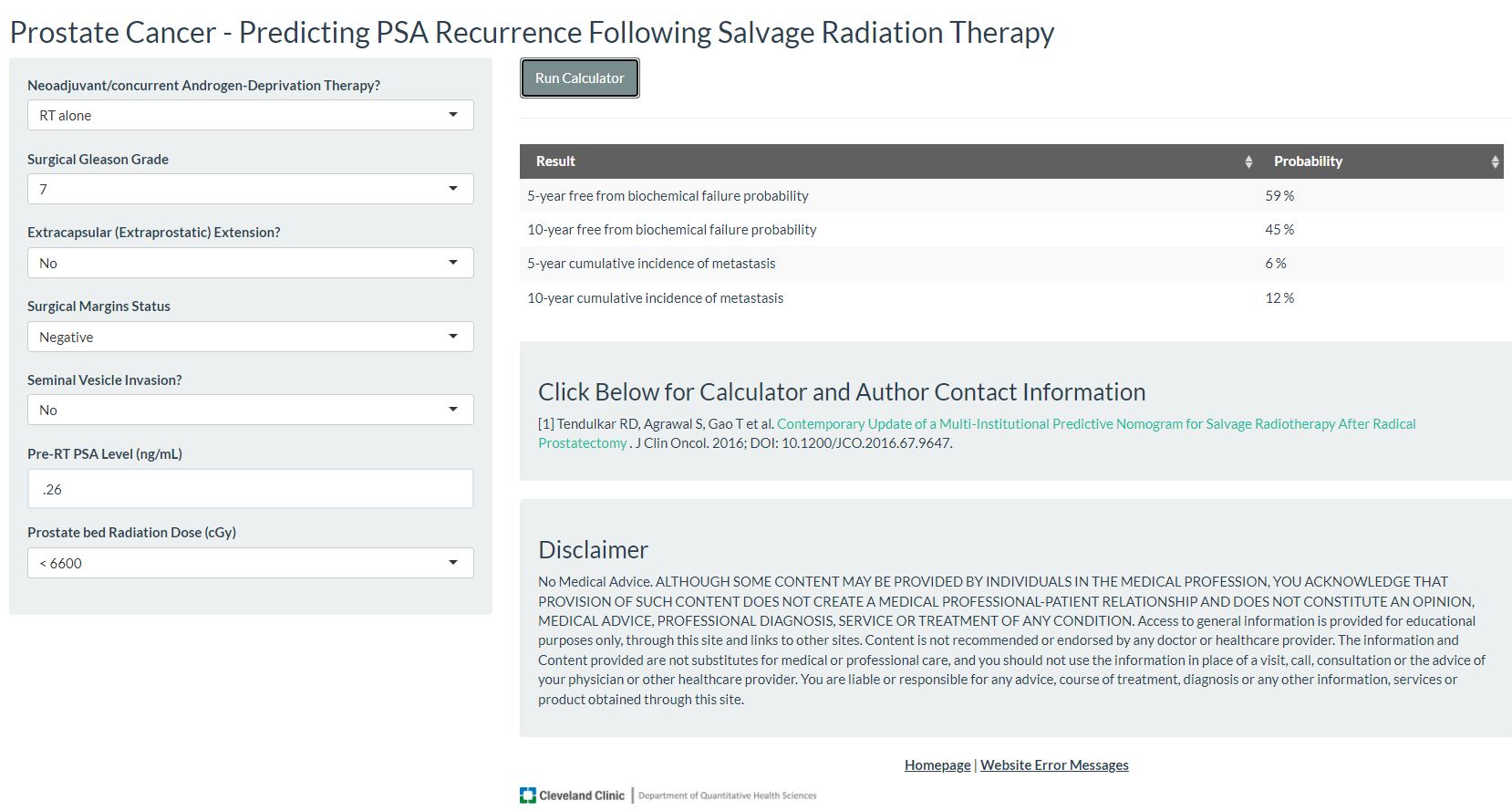
Doing ADT concurrently would give an estimated 10% benefit to the radiation and longer-term PSA reduction according to the doctor. But he also said that my case would also justify doing the salvage radiation alone and holding off on any hormone therapy until after the radiation is completed. He could argue for either option, but was leaning to the more aggressive concurrent therapies.
I asked about the ADT now lessening its effectiveness later when it’s needed most, and he said that six months of ADT would not really make the cancer hormone resistant.
We didn’t do the body mapping this morning based on this little twist, and that’s okay.
He offered to let me contemplate this over the weekend, and he’ll call me Monday morning to answer any further questions and see which option I would prefer.
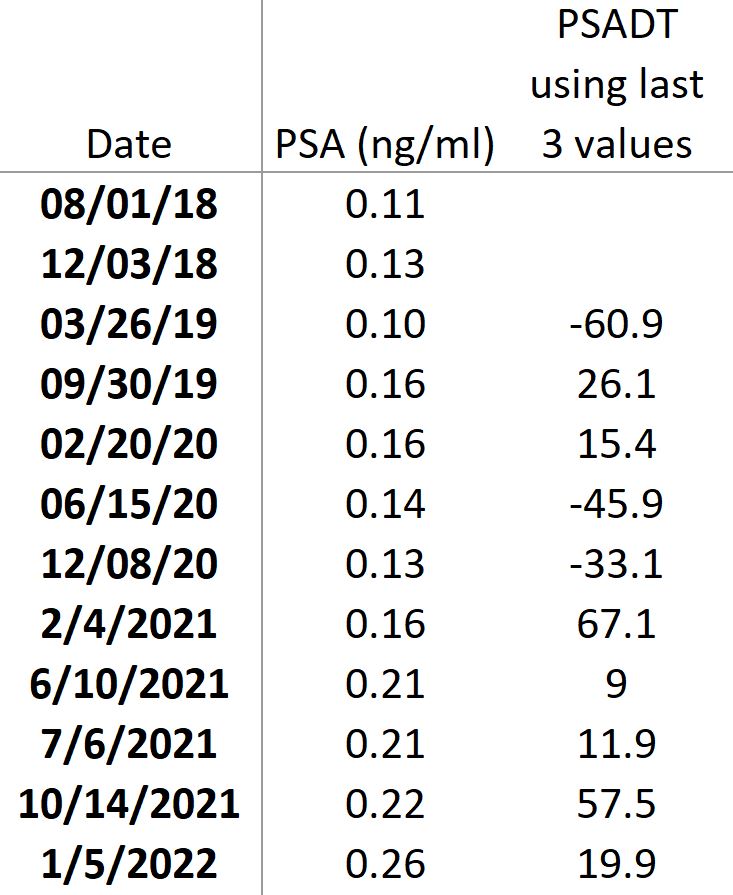
I have to admit that the acceleration in my PSA increases is making me lean toward the more aggressive concurrent therapy.
If I choose the straight radiation, I’d go back to UCSD and get mapped and begin the actual zapping a few weeks later. If I choose the concurrent therapy, I’d have to go back to the VA San Diego for the shot and then wait up to two months (I have to confirm, I wasn’t in the note-taking mode) before starting the actual radiation back at UCSD.
Whichever option I decide, I learned this morning that I’m going to have to practice the art of bladder filling.
I was told for the mapping session that I should come in with a full bladder, so I started drinking water about an hour before the 8:30 a.m. appointment: about half a liter at 7:30 a.m. and another half a liter around 8 a.m., plus sipping on water in the waiting area.
By the time the nurse called me back to the exam room around 8:45 a.m., my bladder was about to burst and I had to run to the toilet. “Try to keep some of it in you,” she blurted as I scurried out the door. Yeah, right. By the time I was leaving after seeing the doctor (about 9:15 a.m.), I had to make another mad dash to the toilet. This has the potential to be pretty tricky.
On a somewhat related note, I needed a bit of escapism in advance of the appointment, and I noticed that the weather in Tucson, Arizona was going to be around 74° F / 23° C the first half of this week. I wanted to head over to spend some time in Saguaro National Park and Organ Pipe Cactus National Monument. It was a hectic trip, but I had fun and it definitely diverted my attention away from all of this.
If you’re interested, you can check out my report and photos here:
Saguaro National Park and Organ Pipe Cactus National Monument