My visit with the urologist this week went about as expected.
We talked about my PSMA PET scan results—negative—and he was of the mindset that those would be the expected results at my PSA level. The scan isn’t reliably sensitive enough when the PSA is hovering around 0.2 ng/ml.
With my steadily increasing PSA, he said that there’s cancer there somewhere. In his view, it’s likely location is still in the prostate bed, but we can’t rule out that there aren’t micro-metastases elsewhere.
In reviewing the totality of my case, he commented, “This is one of the trickier cases I’ve seen.” I don’t believe he was too offended when I replied, “No shit, Sherlock.” I guess my frustration of dealing with this over the years came out a little too strong.
What puzzled him about my case is how long after my surgery the PSA returned and how slowly it was increasing over the years. That led to a discussion about PSA doubling time and how my doubling time is shortening at an accelerating rate.
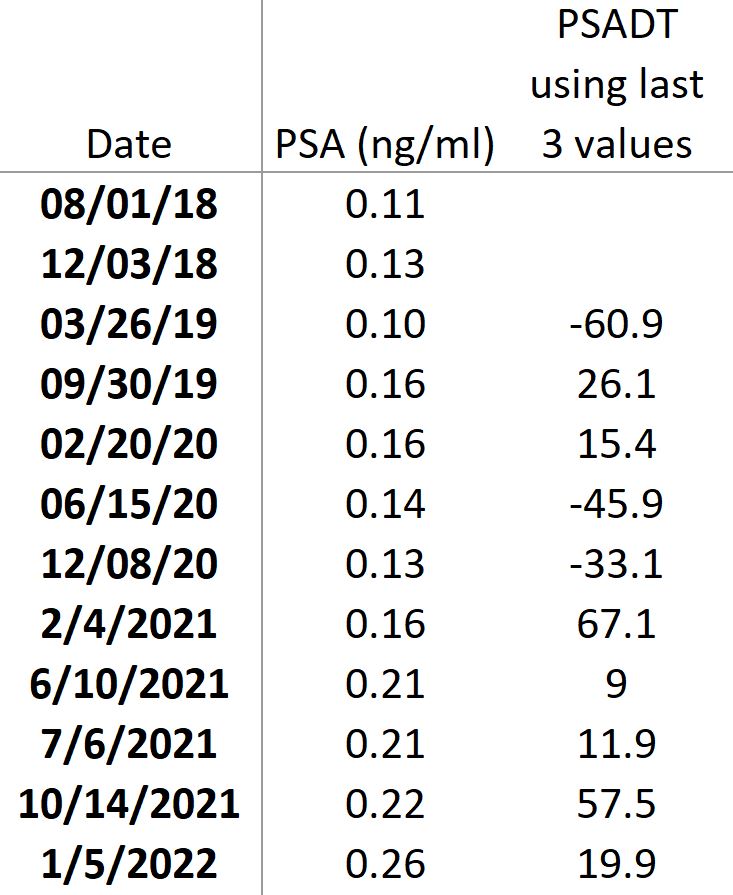
As part of that discussion, I asked him how many data points should be included in the PSA doubling time calculations, and he typically uses only the last three to get a current snapshot of where it is now. (I re-ran my numbers when I got home, and using the last three PSAs, my doubling time is 19.9 months.)
Of course, the engineer in me had to play with that a little, so I went through my PSA spreadsheet and calculated the PSA doubling time if I used the last three values after each test. The results were all over the place:
His recommendation, of course, was salvage radiation to the prostate bed.
He thought that salvage radiation still had a chance of being curative at this point, and given that I’m 64 years old, he thought that I would have plenty of years ahead of me should I choose to go down that path.
We talked about long-term side effects. He thought that there was a 20% to 30% chance that my stress incontinence would worsen, as would my sexual function given where it’s currently at now. He wasn’t confident enough to speak about the chances of rectal issues, at least in the numbers that I was seeking. I expressed concern about the incontinence, and he reminded me that they can take care of that with an artificial sphincter. Great. Another surgery.
I did ask how much longer I could kick this can a little farther down the road, and he didn’t seem to think that that was a good idea at this point. My stomach turned into knots.
We agreed to set up the consult with the radiation oncologist, as well as retest my PSA in early April.
Wednesday afternoon, I received a call from the scheduler trying to set up the radiation oncologist referral. She gave me the option of going to Naval Medical Center San Diego—where I used to work and had a previous referral—or going to University of California San Diego (UCSD). As good a medical treatment facility as NMCSD is, I opted for UCSD. If nothing else than for a second perspective, plus I believe UCSD will have more state-of-the-art equipment and a lower turnover rate in medical teams.
Thursday, morning, UCSD called and we’re set up to meet next Thursday, 17 February 2022. I was a little surprised when they told me that it would be at their Radiation Oncology center that’s about three-quarters of a mile (one kilometer) from my house instead of their main hospital in San Diego.
As you regular readers already know, I’ve been fearful of getting to this point for a while now. Whether my fears are irrational, unfounded or not, I don’t know, but they’re real for me.
My fears center more on having very real, quality of life-impacting side effects from the radiation than on whether or not the radiation will be curative. For some inexplicable reason, my gut intuition is that something will go awry and I’ll be in that 1% or 3% or 10%—or whatever it is—group that gets to experience those side effects impacting quality of life. The radiation oncologist is going to have to give a strong sales pitch to convince me the risks are minimal.
There will be ton of soul-searching and thinking in the days and weeks ahead.
Stay tuned.

Hi Dan, yes it’s a tough one for sure. I had my RT nearly 4 years ago, and I can say that although I’ve had some side effects they are nothing I can’t cope with. Urine incontinence not a problem, ED well that was never great after surgery and didn’t get any worse. The major side effect for me has been bowel urgency but it has settled into a pattern without being too indelicate! Unfortunately my psa has returned as I mentioned in a previous comment but it does seem to have settled atm at around 0.25.
Also, as you know my pet scan came back as yours did NED. Who knows what’s next? You have always had a better doubling time and you’ve got 5 years on me but I’m quietly optimistic atm that the road ahead looks reasonably long at this stage.
Meanwhile I’ve decided to embrace the good times as I’m fit and well, it’s too easy to waste good time worrying about what might be next.
I hope the next stage/decisions are easy for you.
Best wishes
Adrian
LikeLiked by 1 person
Hi Adrian,
Thanks for sharing your experience. I’m glad that incontinence and ED didn’t worsen for you.
I would like to learn a bit more about how you’re defining bowel urgency if you’re comfortable with sharing (I threw delicate out the window on this blog years ago!). Does that mean that you’re still pretty much on a regular schedule, but when the urge to go hits, you have to be within 60 seconds/ 2 minutes/5 minutes of a toilet or there may be a problem? Or are you having increased frequency as well where, just out of the blue at any time of day, you need to make a mad dash to the toilet?
Let’s hope that your PSA remains stable and you continue on in good health for a long time.
Dan
LikeLike
Hi Dan, yes when it comes on there is no waiting.. and stress can increase the urgency, but regular as in same time every morning. I’ve no doubt the RT has damaged my bowel, I get minor bleeding very occasionally and increased mucus which has changed the nature of my movements. It’s definitely not debilitating and is very predictable but a big change nonetheless.
What was also interesting was that the RT definitely hit something as my psa did go back to completely undetectable for a year, my consultant explained this by saying the focal area which was the prostate bed was sterilised but there must have been a margin that didn’t receive the full dose. Micro metastasise? Or is there still some cancer cells remaining in the original site, who knows.. only time will tell.
My next psa is in around a months time, and I’ll have a consultation shortly after. My Onco assures me they will repeat the pet scan when they think it necessary in order to find the recurrence at the earliest possible time, and he says further targeted RT is an option but warned of possible further toxicity to my bowel. My letter says the intent remains curative.
Take care
Adrian
LikeLike
Dan, I think it might be more helpful for you to ask these questions re side effects, at your appointment with the RO. I don’t be,I’ve urologists/surgeons, generally speaking, are as up to date on the capabilities of new equipment technologies, including more advanced software.
FWIW, I have had zero side effects after salvage radiation to the prostate bed as it relates to continence. I do have some mild ED on occasion, but to be fair that started before my treatment.
I am 2 1/2 years past treatment.
And I was surprised when I went for my first post SRT colonoscopy in October and the gastroenterologist told me he didn’t see any signs of radiation damage at all.
I know it’s anecdotal, but I believe it’s largely due to the new technologies (I was on a Varian True Beam machine), and I suppose, to the skill of the technicians.
Good luck at your RO appointment
LikeLike
Hi Ken,
Thanks for sharing your experience. I know there are far more cases like yours out there, but we tend to hear only about the bad experiences. A form of selection bias, I guess.
I agree with asking the RO these questions because, as you pointed out, urologists don’t deal in that field every day and are probably recalling what they learned in school years earlier.
Glad that you’re doing well. All the best.
Dan
LikeLike
Wishing you the best.
Blessings, Richard
LikeLike
Thanks, Richard!
LikeLike
Dan, I had a great experience at UCSD. Another option is proton therapy. It supposedly is more precise and has less side effects. There’s a facility not far from UCSD. The downside is if the cancer cannot be pinpointed all of the additional precision might be a moot point. You might want to go in for a consult though
LikeLike
Hi Scott,
Thanks for sharing. I knew that you had been going to UCSD, so it’s good to hear that it’s been a positive experience for you. I’ll let you know how my experience is.
Dan
LikeLike
Hi Dan. Our two journeys are quite similar in many respects. Like you my quarterly PSA increases jumped around with no consistent pattern other than they were increasing with an average doubling time of 9-12 months. My urologist referred me to a radiation oncologist after my PSA reached .052 in March 2020; approximately 2 years after my RP. The oncologist thought that I would probably require SRT when my PSA reached .200 but there was no urgency and we would continue to monitor my quarterly PSA’s. My consult in April/21 with one of his partners delivered a slightly different message that unless they know where the cancer is located they only have a 50% chance of success and he recommended that we wait until my PSA was getting closer to .400 as long as I was willing to pay for a private PSMA-PET scan; which I was. My urologist disagreed with this approach as my PSA had now reached .210. My research seemed to indicate that the success rate of SRT decreases as your PSA starts to reach 400. By October/21 my PSA had reached .290 and my urologist was pushing me that if I was going to delay the SRT that I should have a PSMA-PET scan to rule out whether the cancer had metastasized, even though it may not identify where the cancer was located. If that meant a second PSMA-PET scan to try to find it; so be it. I did have the scan and the result did show that there was a tiny cancer cell on my seminal vesicle that had been there since the surgery but had not grown very much over the 4 years since surgery. There was no indication of any cancer in the surrounding tissue but the PSMA-PET scan may not have been able to pick it up because my PSA was still relatively low for detection. She indicated that the cancer was not aggressive but it was there and if I wanted to reach my 89th birthday (currently 79) it should be dealt with sooner rather than later. We talked for 45 minutes and I accepted her recommendation of one ADT shot now and I commence SRT in 3 months time along with one more ADT shot. I am comfortable with the decision made and hope that the potential side effects are minor or of a temporary nature. The PC survivor is in a difficult position deciding between delay in hopes of locating the cancer, knowing that the delay in treatment could have negative consequences in eliminating the cancer. Best of luck to you as you proceed on your journey and I do enjoy your posts.
Gary
LikeLike
Hi Gary,
Thanks for such a detailed comment. After 11 years of dealing with this, I’ve realized that there are no black-and-white solutions shared by doctors when it comes to prostate cancer. Each physician has their own approach and recommendations, and that can be frustrating as hell to us patients who are relying on their expertise.
I’ve been thankful for my care through the VA (Veterans Administration) health care system, but each time I go, I see a different doctor. On the one hand, it’s like having multiple second opinions, but on the other, it’s tough to build a relationship and map out a consistent plan/approach to treatment.
I’ve done my research on the success rate of SRT, too, and I’m not keen on the numbers. If I knew that the success rate was going to be in the 85%-90% range, taking on the risk of long-term side effects would be more palatable. But when the likely success rate is in the 65% range, that makes me pause. Why incur life-long side effects for something that won’t succeed?
You may find this nomogram predicting PSA recurrence after SRT interesting: https://riskcalc.org/ProstateCancerAfterRadicalProstatectomyNew/
We’ll see what the RO has to say next week and go from there.
Thanks again for your insights.
Dan
LikeLike
Sending you a virtual hug 🫂 man and wishing you well. At my , now annual, chat with specialist( the surgeon who operated on me) about my 4 year post radical prostectomy PSA result He asked me when we last met and said I was basically cured becauseresult was still less than .001..this before a 5 year remission period. I referenced my knowledge of your experience and will find a different specialist next year.
LikeLike
Thanks for the hug. 🙂 Sorry that you’re feeling that you have to change your specialists. There is something to be said for having that long-term relationship where he knows you’re history, but if you’re not satisfied with the care you’re receiving, then it’s time to move on. I wish you luck in finding a more empathetic replacement.
LikeLike
Hi Dan, I think you are on the right track. My surgeon was very insistent about radiation therapy. However the RO was more conservative, preferring to wait for better evidence of the need before proceeding. Good luck. You will make the right decision for you. Cheers, Phil
LikeLike
Hi Dan have been following you since our gleason #are very close as well as our patholgey reports had radiation @0 14> 6 years after surgery no real problems with the radiation some rectum soreness at the beginning my psa dropped to 0.02 @ 2years later it’s at 0.06…
LikeLike
Thanks for sharing, Jack. Glad to hear that it’s kept your PSA down.
LikeLike
Hi Phil. Thanks for your insights and support. We’ll find out how “gung-ho” this RO is in a few days. Wishing you the best., Dan
LikeLike
Good luck Dan-o. So, the stress is understandable. In the meantime, have faith and perseverate more on “at least at every turn there have been options/ answers”. Certainly, you are not at a place where they have to tell you that nothing can be done. That’s a good thing!!
Pat yourself on the back for a job well done. And keep on keeping on.
?? Steve
LikeLike
Thanks, Steve-o. Hope you’re doing well.
LikeLike
Dan,
FYI…From my experience with Dr. Rose at UCSD – he seems like a rad onc practicing at the top of his license. He might plug in your numbers to the Sloan Kettering estimator to see the difference in probabilities of rad success at .26 versus .4 or .5. Biology is probabilities…but humans are sometimes poor at acting on those probabilities. Please note that Dr. Mark Scholz (med onc with large So. Cal. prostate practice) in his book “The Key to Prostate Cancer” mentions that “some” men can safely wait until .5 before SRT…you might want to check your profile associated with that recommendation.
Regarding Proton…less rad scatter to other areas is their promotion…given that UCSD has some type of association with the SD Proton Center…they will probably head you in that direction for SRT due to your relative young age.
Truly hope you make good choices for yourself…wish you the best…
Max
LikeLike
Hi Max,
Thanks for your suggestion. I ran the MSKCC nomogram at 0.4 ng/ml and the probability of progression dropped from 64% at my current PSA of 0.26 to 63% at 0.4. In other words, no real difference.
Also, you may want to jump into this video (at the 3:40 mark) from Dr. Scholz who says that they’re not seeing a substantial difference in side effects from Proton therapy vs. IMRT.
Thanks again.
LikeLike
Dan,
Thanks for the Dr. Shultz video…as mentioned – Dr. Shultz might recommend you wait on RAD until .5 given your profile…it is in his book and he discusses it on one of his videos about recurrence. I know much of what you are currently going through at this juncture…I am “roughly” where you are at with BCR after 5 years and a PSA now at .2 with a PSADT of about 33 months – Ga PSMA PET/CT in December that showed nothing. I have become somewhat informed…reading everything I can and seeing a number of doctors. Very scary time for me…at this point – I will probably wait until .4 for another PSMA PET/CT with the hope of targeting something. I know there is a risk to wait…but getting in the car every day has risk. If you every want to have coffee to compare notes and strategies…just let me know – because I live in your city. Regardless – please keep posting because I value your insights…you have helped me greatly…if I see anything of interest – I will send it your way.
Best – Max
LikeLike
Dan – it’s a tough call you’re facing. Everybody’s decision is their own. If you decide to go ahead with the SRT you might find my blog useful. Best to start from the beginning in March 2016. https://crossingthertquarter.wordpress.com. Keep going – its a long road!
LikeLike
Thanks, Simon. I’ve actually seen your blog before, years ago, and I’ll take some time to go through your posts.
All the best!
LikeLike