I just received a quick update from my health insurance company regarding coverage of the Ga68 PSMA PET scan at UCLA—the quick turnaround surprised me. It appears to be good news, but it was a little squishy, so I had to ask for confirmation of a few things.
In their email to me, they listed the contractual amount that they would pay out for each CPT code that I gave them, but that’s all they said. It sort of implies that I’m covered, but it doesn’t say so explicitly. Needless to say, when dealing with insurance companies, I want things to be very explicit without any loopholes.
I just sent them and email asking them to:
Confirm that I am covered under my employer-provided healthcare plan.
Confirm whether or not UCLA Department of Nuclear Medicine is considered to be in-network or out-of-network (different deductibles).
Hopefully, I get that confirmation early next week and can share the information with my doctor.
My health insurance company replied to my email with more questions than answers, which was okay by me because they were trying to learn more about the Ga68 PSMA PET scan at UCLA.
First, they were looking for the Current Procedural Terminology (CPT) codes that would apply to the imaging. I didn’t know what those were, so I had to do a little searching:
Current Procedural Terminology, more commonly known as CPT®, refers to a medical code set created and maintained by the American Medical Association — and used by physicians, allied health professionals, nonphysician practitioners, hospitals, outpatient facilities, and laboratories to represent the services and procedures they perform. No provider of outpatient services gets paid without reporting the proper CPT® codes.
I was able to schedule my bone and CT scans this morning with considerable ease. In fact, things will happen much sooner than I thought they might. My CT scan is scheduled next Wednesday, 14 July, and my bone scan is scheduled Friday, 23 July.
I have to go for some pre-scan lab work tomorrow afternoon to ensure that my kidneys are working fine and won’t be damaged by one of the contrasts.
I haven’t given up on the Ga-68 PSMA PET scan. In fact, I wrote my health insurance company an email about 4:30 a.m. as I tossed and turned. (Last night was hell. If I slept more than 2 hours—non-consecutively—that was about it.) They tout having a response within 2 business days, so we’ll see if they come through with that.
UCLA is out of network for my insurance company, so I’d have to cough up 40% of the cost if they’re going to cover it at all. I’m okay with that. (For my overseas readers, welcome to U.S. health care systems!)
So that’s the latest and greatest. More to come, I’m sure.
Anticipation for this appointment really did a number on me for some reason. I was nervous to the point of feeling queasy as I was driving to the San Diego VA Medical Center, which is quite unusual given how many times I’ve done this. I guess that this was different because my PSA had broached that dreaded 0.2 ng/mL mark.
Okay. I started this post (above) while sitting in the waiting area waiting for my appointment, and afterwards, my plan was to sit down at home this evening and summarize what we discussed. But the doctor just called a few minutes ago with some information that completely changes how I’m going to approach this post.
PSA Results
In a nutshell, one of the things we discussed was re-running the PSA test to see if last month’s 0.21 ng/mL was a real reading, or if it was an anomaly like the February 2020 drop from 0.16 ng/mL to 0.08 ng/mL. She even asked me if I had had an orgasm or rode a bicycle or did other similar activities before the June test. I had done none of those.
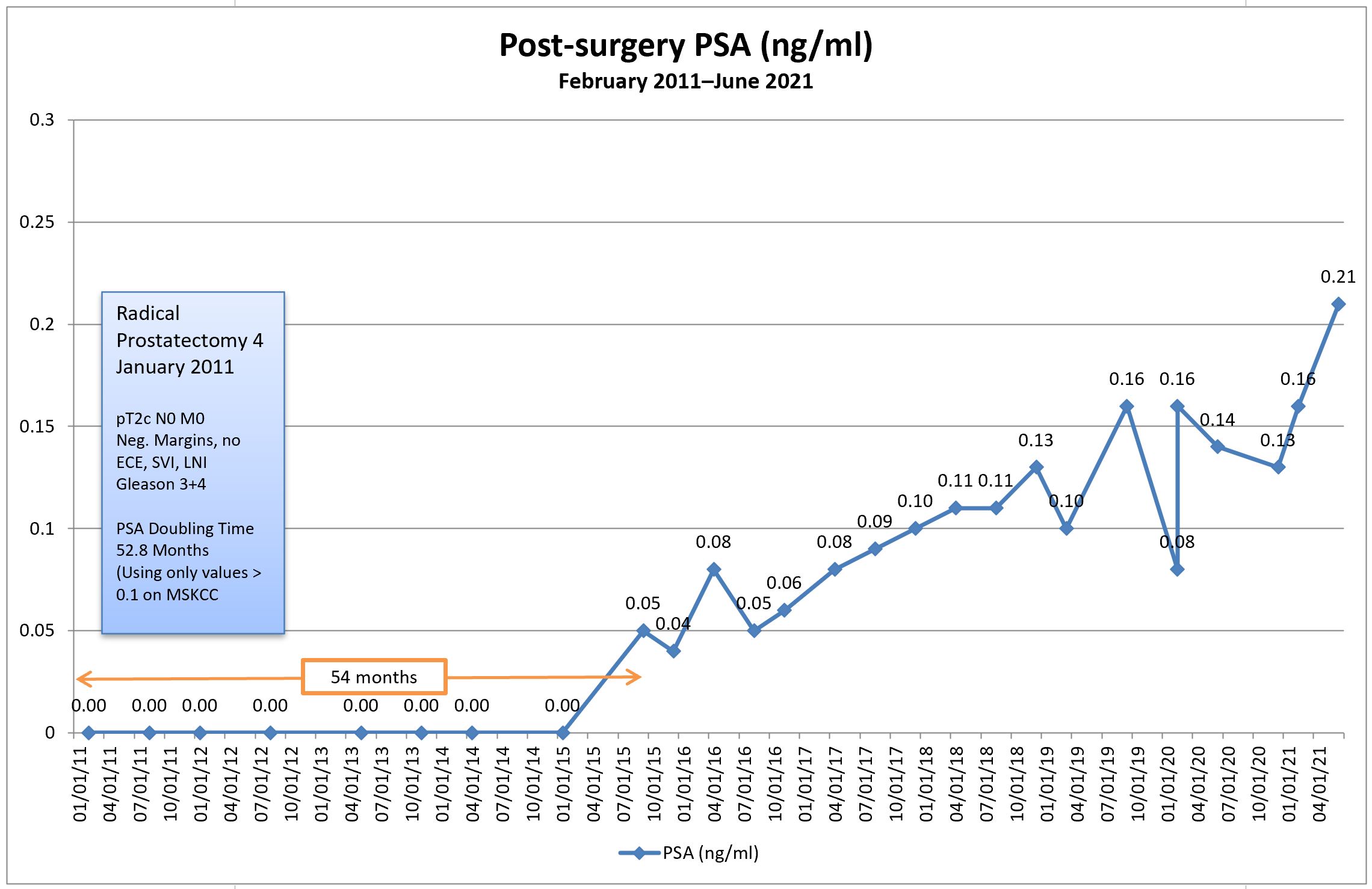
I asked to have the test re-run for peace of mind and she put the order in the system. She said that she should be able to see the results later this afternoon before they’re posted online, and instructed me to call her later in the day. She just returned my call with the results: my PSA came in at 0.21 again, confirming the June result. (You can also see that my PSA doubling time dropped to 48.1 months from 52.8 months in June.)
Note the addition of PSA doubling time to the chart in red, showing the PSA doubling time in months (right axis). [Click chart to enlarge.]
I’m not pleased that I’m hanging out in the 0.21 range, but I am pleased to have the confirmation. Now we know what we’re dealing with.
Plan A
During the consultation, we talked about possible courses of action. The first was to get the results and, if they were still hanging in the 0.16-0.18 range, we’d continue to monitor, perhaps bumping the frequency of PSA tests to three or four months instead. Obviously, that plan got tossed out the window.
Plan B
If the PSA came back with a confirmatory value, we agreed that scans to try to locate the cancer would be an appropriate next step. That was a great opening for me to talk about the Ga-68 PSMA PET scans at UCLA, but more on that later.
One thing that I’ve noticed in my years of being cared for at the VA Medical Center is that they do seem to be a tad slower to embrace some of the new technologies, definitions, and treatment options that are out there. Their protocol for someone in my situation is a bone scan in combination with a CT scan, so that’s what I’ll be calling to arrange tomorrow.
I argued that it’s very unlikely that the bone scan will pick up anything at my PSA level, and my doctor’s response was that we might be surprised. Ditto for the CT scan. If both scans are negative, the protocols would allow us to proceed to an Axumin PET scan done at the VA Medical Center. If the Axumin PET scan came back negative, then we may be able to figure out a way to get the PSMA PET scan at UCLA.
Of course, my preference would be to go straight to UCLA and skip the bone, CT, and Axumin scans altogether, but if those are the protocols that may get me answers I’m seeking, then I guess I need to follow them. Even so, I may try to push for the PSMA PET in place of the Axumin (I even mentioned to her that I may be willing to pay for it myself if the VA and my own insurance didn’t cover it).
General Conversation
One of the questions that I asked was about when the actual PSA value trumps the PSA doubling time when it comes to deciding to take action. Clearly, each case is unique and there is no definitive answer, but my doctor’s take on it was that she wouldn’t let a PSA go above 1.0 ng/mL without taking some action.
She did, however, bring up the fact that it’s becoming more widely accepted to do exactly what I’ve been doing—continuous monitoring. Too many patients are being overtreated with salvage radiation therapy with no guarantee of it being curative. She referenced how the American Urological Association (AUA) and National Comprehensive Cancer Network (NCCN) guidelines have been evolving over the years in a way that supports monitoring over action in some cases.
When I brought up the Ga-68 PSMA PET scan, it seemed that I may have been a little more up to speed on the topic than she was. We talked about it being FDA approved at UCLA and she reminded me that, just because it’s approved doesn’t mean it’s covered under the VA or private insurance yet. I agreed, and that’s when I mentioned I may be willing to pay for it myself.
I brought a hard-copy of this paper on the Ga-68 PSMA PET scan and left it with her for her review. We also reviewed the chart showing what the scan was picking up at various PSA levels, and where it was picking it up.
I found it interesting that one of the first things she looked at with the paper was who the authors were. I guess quacks write papers, too.
Final Thoughts
It’s been one helluva weird day, that’s for certain. It started with me feeling uncertain and queasy and, in a bizarre twist, I feel as though I’m ending it on a high note.
Sure. No one wants to have recurrent cancer. It sucks. But now I feel the uncertainty brought on by PSA results bouncing around for the last six years is finally coming to a close, and I can really begin to focus on what happens next. There’s a sense of direction, albeit down a path none of us would like to go down. (Yes, there’s lots more uncertainty ahead, I’m sure, but I’ll cross that bridge when I get to it.)
Tomorrow I’ll call to get the bone and CT scans set up and, once we know the dates, I can arrange a follow-up appointment to review the results.
If they come back negative, then we try the Axumin or PSMA PET scan if possible. Of course, I’ll be doing some reading on Axumin scans in the interim (I really haven’t focused that much on them as an option, so I need to learn more about them).
Having cancer sucks. Having more definitive information doesn’t.
This is a really interesting (at least to me) video out of the University of California San Francisco (UCSF). Remember that UCSF and UCLA were the two institutions that did considerable work to get the Ga-68 PSMA PET scan approved by the Food and Drug Administration in December 2020.
First, at the 3:04 minute mark in the video, he presents the number of positive scans by PSA level. Interestingly, he references the same study I posted earlier. What differs in this presentation from the other one I posted is that this looks at PSA values <0.2 and from 0.2-0.49, whereas the other study just looked at positive scans for PSA values <0.5. However, something seems off between the two.
In the original study, it showed a positive detection rate of about 38% for PSA values <0.5. In this video, however, the chart appears to show a positive detection rate at the <0.2 PSA level somewhere north of 40%, and a positive detection rate at the 0.2-0.49 PSA level somewhere north of 50%. Perhaps he wasn’t all that skilled at making bar charts in PowerPoint, but something is amiss.
Where I’m encouraged is that it appears that they are, in fact, able to detect cancer at my PSA level or even lower. The only question is, at what rate? I’ll stick with the one in three value for now, which is still better than zero.
I did email one of the doctors on the team at UCSF, and his response was:
There are no guarantees, but there is a chance that a PSMA PET could detect a site of recurrence with a PSA of greater than 0.2. The chance of detection usually increases as the PSA goes up.
Not exactly a ringing endorsement of his own product, but I think that’s more to couch expectations because this is so new and even he is still trying to figure it out. (I admit, I was surprised that he even responded, so I’m thankful for that.)
I’ve got a good list of questions ready for my appointment on Tuesday, and I’m sure I’ll spend some of this holiday weekend adding to it and refining it.
I came across this video highlighting Ga68 PSMA PET imaging from the doctor at the University of California San Francisco who helped with developing this imaging technique. It’s a bit long and a bit technical in some places, but gives a good overview.
Today was a tough day. The news of my PSA increasing to 0.21 ng/ml weighed heavily on me throughout the day. It even made me a little snippy in a meeting this morning, as my tolerance for trivial bullsh*t decreased to an all-time low. Oh well. They’ll get over it.
Long-time readers of this blog already know that I’ve delayed starting salvage radiation therapy because I’m reluctant to incur the short- and long-term side effects of radiation without having a higher degree of confidence that we’re actually zapping in the correct location(s)—zapping the cancer itself.
Of course, the current state of imaging for prostate cancer generally sucks, but it is getting better with advances like PSMA PET scans using 68Ga-PSMA-11 where prostate cancer can be located much earlier and much more accurately than using previous technologies such as bone scans. But even 68Ga PSMA PET scans have their limitations.
One of the greatest challenges (gambles?) in deciding when to start salvage radiation therapy is the timing. Most will argue the earlier, the better. Statistics show that in most cases, the cancer is still in the prostate bed or pelvic region, so the radiation oncologists start blindly zapping those regions hoping the statistics are correct. But the cancer could have already spread to more remote locations.
With my PSA doubling time in the 4-5 year range, my team and I have decided to hold off on salvage radiation therapy and, in so doing, I’ve avoided any radiation side effects for five years giving me a high quality of life during that time. That has value to me. Of course, none of us know whether the little buggers have been hanging out in the prostate bed during that time (like statistics would show), or if they’ve gone on one of their own infamous road trips and have started spreading.
One of the things that I’ve been trying to determine for months now is at what PSA level can the Ga68 PSMA PET scan begin to reliably pick up prostate cancer. The answer typically was in the 1.0 to 2.0 range for the PSA. With a PSA a fraction of that (0.21) the PSMA PET scan really wouldn’t be a reliable tool for me yet. It’s not a completely worthless tool, but there are decent chances that I could come away with a false negative result.
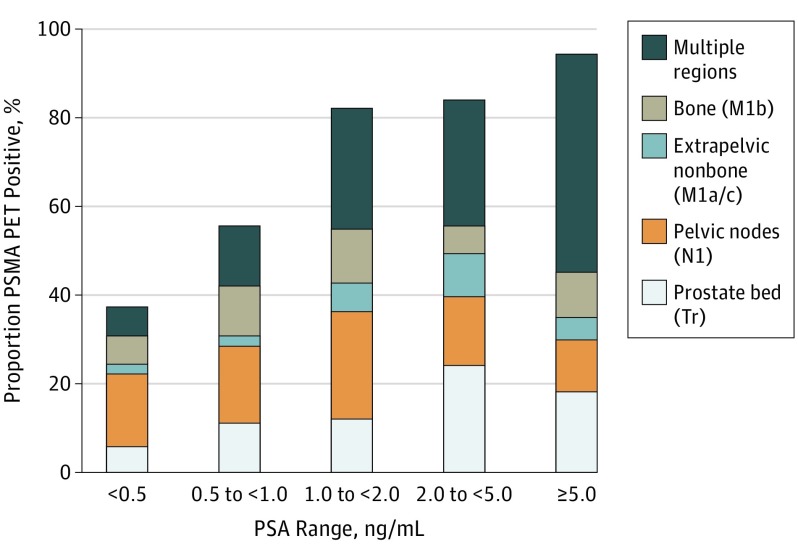
The chart below taken from the paper was exactly what I was looking for and more. First, it shows the number of cases where patients with an increasing PSA after prostatectomy have positive results based on their PSA level. For those with PSAs less than 0.5 ng/ml (me), the number of positive cases was only 38%. In other words, there’s about a one in three chance that the Ga68 PSMA PET will be able to locate the cancer at that PSA level. Not good odds, but better than zero.
To me, the really interesting thing about this chart is that it shows the location of where the PSMA PET scan found the cancer by PSA level.
Fendler WP, Calais J, Eiber M, Flavell RR, Mishoe A, Feng FY, Nguyen HG, Reiter RE, Rettig MB, Okamoto S, Emmett L, Zacho HD, Ilhan H, Wetter A, Rischpler C, Schoder H, Burger IA, Gartmann J, Smith R, Small EJ, Slavik R, Carroll PR, Herrmann K, Czernin J, Hope TA. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019 Jun 1;5(6):856-863. doi: 10.1001/jamaoncol.2019.0096. PMID: 30920593; PMCID: PMC6567829.
You can see that more than half of the cancer in patients with PSAs below 0.5 were found either in the prostate bed or pelvic region, both of which should be very treatable with salvage radiation therapy.
However, once the cancer is in other the other regions—extrapelvic nonbone (other organs), bone, or multiple regions—the cancer becomes very difficult if not impossible to treat. At that point, it’s only managed.
Please keep in mind that those are my non-expert opinions that I will have to confirm with my medical team to make sure I’m interpreting things correctly.
You can see that, as your PSA increases above 0.5 ng/ml, the cancer was found more broadly in the study participants. By that, I mean the cancer had spread beyond the prostate bed and pelvic region. You can also see, however, that even with PSAs less than 0.5, the cancer has already spread elsewhere in about 40% of the patients in the study with that PSA level.
That’s the whole point of knowing this. If the cancer has already spread, there’s no sense in zapping the prostate bed or pelvis risking long-term radiation side effects adversely impacting quality of life for no gain whatsoever.
This is only one study with 635 patients, so I am taking the results above with a healthy dose of skepticism, and I’ll continue to do more research in the three weeks before my appointment. But this study will be a good conversation opener for the consultation.
Some of the questions that are on the top of my bald head are:
Should we run another PSA test to see if this was an outlier/anomaly like some of my previous PSA tests (I’ve been using the same lab all along)?
How much weight does PSA doubling time have now that we’ve crossed the 0.2 ng/ml threshold?
Would he support getting the Ga68 PSMA PET scan done at this PSA level?
If not, at what PSA level would he support getting the PSMA PET scan?
Would he be willing to give me a referral to get one done even if I have to pay for it myself?
Fortunately, the US Food and Drug Administration approved the Ga68 PSMA PET scan at the University of California Los Angeles (UCLA), and that would be a 2.5-3 hour drive for me to get up there to have the scan.
In the meantime, I’m going to have to reconcile in my own mind how high I’m going to let my PSA get before taking action, scan or not.
Lots of research, thinking, and soul-searching ahead. But be forewarned: My trivial B.S. tolerance level is way less than my PSA. 🙂
I went for my originally scheduled six-month PSA test last Thursday and was able to look online last night to see the disconcerting results: A substantial increase to 0.21 ng/ml.
Breaking the 0.2 ng/ml threshold now officially puts me into the biochemical recurrence category, at least according to the long-held definition of biochemical recurrence.
Needless to say, I felt gut-punched on seeing the results. Sure, I’ve know for over five years that my trend has been upward, but I guess I got comfortable with it bouncing around the 0.10 to 0.16 range for the last few years. I wasn’t expecting such a substantial leap between my “surprise” PSA test in February and this one in June.
When it comes to PSA doubling time, it dropped from 67.7 months to 52.8 months with this latest test result included in the calculations. If I look at only the five most recent test results, the PSA doubling time drops to 46.5 months. Of course, all of those are great numbers that a lot of guys would like to have.
My appointment with the doctor isn’t until 6 July, and it will be an interesting conversation now that we’ve crossed that magical line of 0.2 ng/ml. In a way, I’m glad I’ve got several weeks to think this through and to come up with good questions to ask so that I’m prepared for the appointment.
Of course, salvage radiation therapy just moved to the top of the list of things to talk about. It will be interesting to see if their recommendation changes given the 0.21 number versus the long PSA doubling time.
Needless to say, there’s going to be much reflection and research in the weeks ahead.
In ,a recent media release, Lantheus Holdings announced that the US Food and Drug Administration (FDA) had approved the imaging agent known as piflufolastat F 18 Injection (also known as Pylarify® or more commonly just “PyL”) as a PSMA-based PET imaging agent for identification of prostate cancer. This agent is actually approved for use in […]