Before getting into the conversation with the urologist, I went for my bone density scan last week. The results? I have bones. They’re dense (i.e., normal). Now we have a baseline for future reference for if and when I start down the hormone therapy path.
Yesterday’s meeting with the urologist was unusually animated, if not bordering on contentious. The appointment was late in the afternoon (around 3:45 p.m. when she arrived), so perhaps she had had a crappy day and was ready for it to end.
I tried explaining my conversations with both oncologists, and she kept interrupting, sometimes with questions that made it seem that she wasn’t paying much attention. (She was on her computer reviewing my file as I talked; usually she’ll have reviewed the file before even walking into the exam room.)
At one point she said, “You have three cooks in the kitchen and should probably stick with one,” referring to the fact that I had two oncologists and her trying to manage my case.
When it comes to treatment, she’s still of the opinion to wait until metastasis to start hormone therapy, mainly because of the associated side effects and possible earlier resistance to the therapy. I mentioned that both oncologists recommended intermittent hormone therapy, and she seemed puzzled by that for some unknown reason.
I mentioned that the plan was for me to have another PSA test in the first week of September and, if warranted, a CT scan and bone scan in December. She seemed indifferent and offered no comment one way or the other.
By the end of the appointment, it was pretty clear that she was of the mindset that there’s little that she as a urologist can do at this point in my case management, and that the ball belongs squarely in the court of the oncologists. I agree. She did say, though, that if I start to have urinary symptoms that may be from the radiation or surgery (e.g., strictures, worsening incontinence), to come back to Urology for investigation and possible treatment. We did not set up a follow-up appointment for Urology.
Back in April, the oncologist suggested they take the lead on my case and, after yesterday’s appointment with the urologist, it’s clear that that’s what needs to happen.
I’ve got the PSA test on my calendar on 2 September. We’ll get the results, calculate PSA doubling time, and consult with the oncologists to determine the next steps based on the results.
If my PSA shoots up again like it did between December and March, reducing my PSA DT, I might be more inclined to act. But if it continues on a flatter trend like it did between March and May, I’d be inclined to kick the can down the road another three months.
So I’ll continue to live life in three-month increments until the results tell me it’s time to do something. Good thing I have a lot of hurry-up-and-wait experience from the Navy. 🙂
My visits with the medical oncologists yesterday and today went well, and there was some consensus on how to proceed.
[BLUF: We’re kicking the can down the road three months.]
UCSD Oncologist
The first part of the meeting was getting the doctor up to speed on my case, as he didn’t have any of the history. Of course, nerd me came prepared with a two-page Reader’s Digest chronological summary of my diagnosis and treatment, printouts of my PSA charts, and copies of the PSA doubling time (PSA DT) calculations.
PSA Doubling Time
Because PSA DT is an important number in the decision-making process, I opened the conversation by asking him how many data points should be used in the calculations. He chuckled a bit before saying that one of the downfalls of using PSA DT is you can pick and choose the data that you want to get the answer that you want. So true.
I calculated my PSA DT using 3, 4, and 5 values and came up with different answers:
Number of values used
Going back X months
Calculated PSA DT
3
6
7.6 months
4
9
8.0 months
5
14
9.2 months
He just looked at the curve on my PSA tracking chart and estimated in his head that it was around nine months. In his eyes, that six to nine month PSA DT warrants closer observation and monitoring.
Inconclusive PSMA PET scans
We discussed my four inconclusive PSMA PET scans and [F18] FDG PET scan, and whether he thought that I was PSMA negative. He thought it was unlikely that I was, offering up a case with another patient whose PSA was over 50 ng/mL and still showing up negative on PSMA PET scans.
One of the reasons that we talked about that at some length was that he suggested that Pluvicto / Lutetium-177 might be an option.
I asked about getting an Axumin scan or a Choline-11 scan, and he wasn’t in favor of doing either of those at the moment.
When to Start ADT
We also discussed when to start androgen deprivation (hormone) therapy (ADT). He didn’t have a set of specific criteria that he would use—e.g., specific PSA number, evidence of metastasis—but did focus in on the rate of PSA rise (PSA DT) and “patient motivations and preferences.”
What type of ADT
The doctor was a proponent of intermittent therapy in my case with six to twelve months on, then a similar period off. His goal would be to “maximize time off treatment” as long as my PSA is holding relatively steady and not going bonkers.
He seemed a tad hesitant to start with the combination therapy of ADT + ARPI (Eligard + Enzalutamide), but wasn’t opposed to it, either. He wasn’t a fan of trying the Enzalutamide alone because of its side effects (gynecomastia, in particular) and not seeing any substantial changes in long term outcomes.
Summary
I did share with the doctor the VA MO’s desire to start ADT + ARPI sooner rather than later, and he had a much lower sense of urgency in taking action. And, while I was a bonehead and didn’t explicitly ask him for his recommended course of action, the entire conversation led me to conclude that his preference was for continued close observation.
VA Oncologist
I technically didn’t meet with the oncologist; I met with a nurse practitioner who had reviewed my case with the oncologist just before (and during) my appointment.
Discussion
It was interesting that she opened the conversation with a quick review of my last appointment there, told me my PSA results from last week, and then said something along the lines of, “If you’re not ready to start ADT today, the doctor is okay with monitoring for another three months.”
At that point, I mentioned that I went to the UCSD MO the day before, and I spent a good chunk of time relaying how that meeting went.
I reminded her that I have the bone density scan in a few weeks and I intended to go through with that to establish a baseline even though we might not start ADT right away. She agreed.
I’m still meeting with the VA urologist on 23 June and want to get their thoughts on what’s next.
Summary
We’re going to do another PSA test in September, and the VA MO didn’t want to schedule an appointment with me until December with another PSA test just before that meeting, too. Interestingly, the VA MO also wanted to schedule a regular CT scan and bone scan ahead of the December appointment.
However, if the September PSA test jumps up significantly, we’ll revisit that plan based on the results. That may change doing the CT/Bone scans to another PSMA PET scan.
The Plan
In short, we’re going to kick the can down the road another three months.
More specifically:
Bone density scan – 17 June
Urologist appointment – 23 June
PSA test – First week of September
CT and Bone scan – First week of December
PSA test – First week of December
VA Oncology Appointment – 8 December
Summary
On the whole, I’m pleased with the plan as it stands right now. The UCSD MO emphasized the shared decision-making approach, adding in his notes, “Daniel is very well educated about his illness and understands there is no clearcut right and wrong answer.” Ain’t that the truth (about the no right or wrong answer).
Once I cleared the hurdles of getting set up in the UCSD system, I was impressed by the friendliness and professionalism of their staff in the department. They have a patient portal app that allows access to records and makes communicating about appointments—in both directions—quite easy.
One thing that I’ve noticed with both the VA and UCSD oncology departments is that their empathy and caring nature seems to be a notch or two above that of their respective urology departments. Not that the urology teams aren’t caring or empathetic; it’s just that the oncology folks seem to take it a step further.
I know the VA MO expressed a desire to take the lead on my case at my last appointment, and I’ll mention that to the urologist on the 23rd. And, for now, as pleasant as the experience at UCSD was, I plan on having the VA be my primary source of care.
I went for my PSA test this morning and already have the results this afternoon (a pleasant surprise).
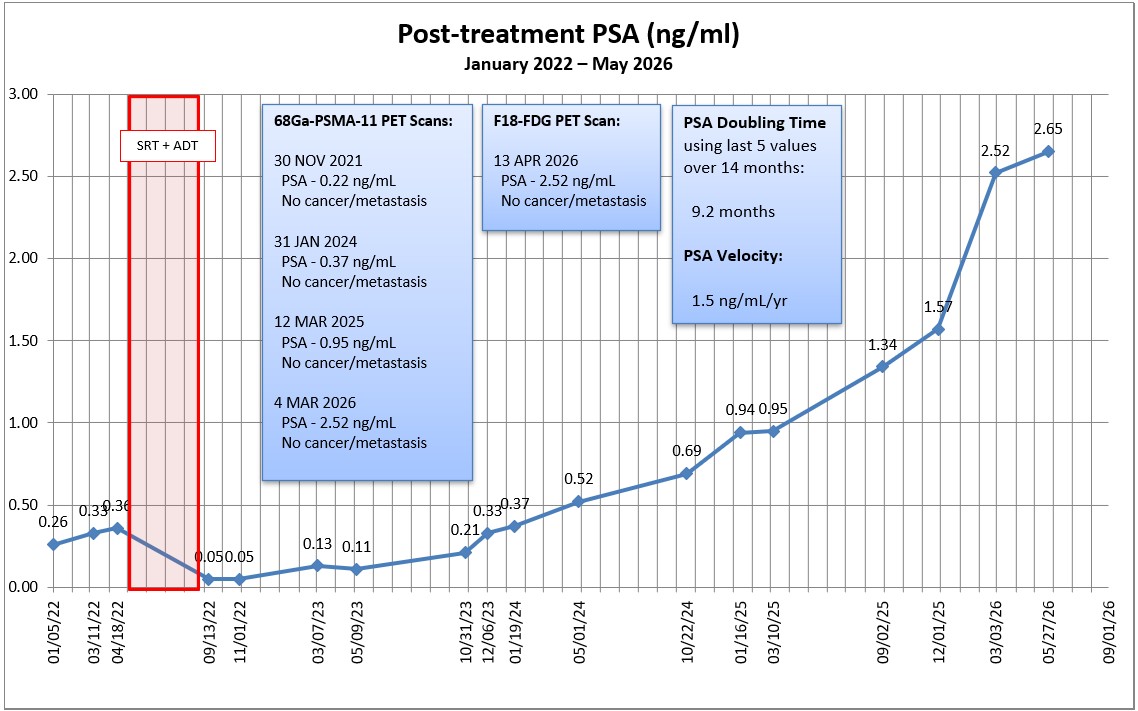
My PSA increased, but not as much as I expected it to. It went from 2.52 ng/mL in March to 2.65 ng/mL today.
If I use the last five PSA values to calculate PSA doubling time going back 14 months, my PSA DT is 9.2 months. If I use the last four PSA values going back only nine months, it’s 8.0 months. Again, the VA medical oncologist used the nine month PSA DT one of the triggers to start hormone therapy.
Armed with these latest results, I should be ready for my upcoming appointments:
Monday, 1 June – UCSD Medical oncologist
Tuesday, 2 June – VA Medical oncologist
Wednesday, 17 June – Bone density scan to establish baseline
Tuesday, 23 June – VA Urologist
I definitely plan on asking the UCSD MO what his thoughts are on an Axumin scan, and whether it’s worth pursuing before we start hormone therapy. If he agrees, I’ll have to add that to the schedule, too.
I also had another testosterone test done to establish a baseline should I opt to start hormone therapy. It came in at 416 ng/dL (reference range 200-800 ng/dL).
Over the holiday weekend, UCSD sent an automated email asking me to complete their electronic check-in process. Sheesh. It took more than an hour of filling out forms, providing history, and updating insurance. The only thing they didn’t ask for was our family cat’s name from when I was five years old. Hopefully, getting all that taken care of in advance makes the appointment go more smoothly.
We last left our hero with the beginning of a head cold after his scan and oncologist meeting. And, boy, what a head cold that turned out to be.
Normally, a typical head cold lasts a week or so and you’re back to normal. Not this time. This was the most stubborn virus, hanging on for three weeks and change. It was ugly. So ugly, in fact, that I went to the doctor for help.
The cold started out with a light fever and lots and lots of coughing. Of course, when you have your prostate plucked from your pelvis and they zap what’s left, stress incontinence is an issue. If I have a light cough, I’m generally okay, but with this virus, I was having deep coughs where it seemed as though I was trying to turn my lungs inside out. I had to switch to the heavy-duty incontinence pads and, even then, I blew out two of them with coughing fits, leaking into my underwear and jeans. Messy and not fun.
The doctor gave me something to calm the dry coughs, and that had a bit of a positive effect. But then my sinuses filled, my nose was running, and I was coughing up phlegm so I switched to something else to deal with that.
Long story shorter, it’s pretty much all behind me now, and that’s a good thing. Maybe I’ll go back to the COVID days and wear masks when riding packed transit or wandering the halls of hospitals.
While I was down for the count, I had plenty of time to dig into more about androgen deprivation therapy (ADT), its pros and cons, and the timing of starting it. Sadly, I could find information that supported pretty much any perspective you wanted, which really isn’t all that helpful.
On the whole, it appears the current thinking is to start ADT sooner rather than later, and to use a doublet therapy, i.e., ADT + ARPI. This seems to delay time to metastasis, but has the obvious cost of substantial side effects.
On a related note, I called UCSD on 30 April to set up a second opinion appointment with the medical oncologist that’s well-respected and that the VA called to consult on my case two years ago. Because I was already in their system, that helped a little. I had to update my insurance information, and they said they’d get back to me in 2-3 business days. They didn’t, so I called back today, 11 May. They put me on the “high priority” call-back list this afternoon to be called back “between now and 48 hours.” Okie-dokie. And they say scheduling appointments at the VA is difficult…
I’ve got a number of appointments coming up at the end of May and into June:
27 May – PSA Test and other pre-ADT labs ordered by the oncologist
2 June – Meeting with VA medical oncologist
17 June – Dexa Scan bone density scan for baseline
23 June – Meeting with VA urologist
With luck, I’ll be able to add the UCSD medical oncologist to that list as well.
I really want the PSA test results—specifically, the PSA doubling time—to be a guide into what happens next and when.
One of the other things that I dug into a bit when I was down with the cold was how many values to use when calculating PSADT. As expected, there were dozens of different answers. Grr. My pea-sized engineer’s brain decided that I’ll use the last four PSA values if they cover at least a year. To me, that would render more useful information that shows the latest trend versus loading in all data points that may skew the results to show something less aggressive. But what do I know?
Using the Memorial Sloan-Kettering PSADT calculator and four data points over the last year, my PSADT is 8.9 months. Using a second calculator I found, it’s 8.21 months. For grins and giggles, I plugged in the last two years worth of data, and my PSADT was 10.4 months. Doing my research on ADT, PSADTs in the 6-9 month range seemed to be a trigger for action.
My PSA in March was 2.52 ng/mL, and I suspect it will be approaching 3.0 ng/mL at the end of May.
Obviously, this summer will be a series of data collection, evaluation, and big decision-making. Yippee! <sarcasm font>
I had my post-PSMA PET scan visit with the urologist today, and I wasn’t really sure what to expect going into it.
The doctor (same as last time) shared the scan results saying that they’re something I should celebrate. I mentioned, though, that I have had three scans and were inconclusive despite the rising PSA numbers. He was quick to reply by saying that the scan not showing evidence of prostate cancer or metastasis was conclusive.
I understand where he’s coming from, but until we know where the cancer is, I’m going to have a difficult time accepting that perspective.
I did ask whether there was some sort of test that can determine if my cancer doesn’t express PSMA, and he said that there wasn’t. Something in my pea-sized brain tells me I need to double check him on that.
I also asked if there could be another explanation beyond the cancer that would explain my rising PSA. He ruled out the possibility of some residual prostate tissue being left behind after the surgery as being the cause based on my PSA kinetics over time.
In terms of what’s next, we’re kicking the can six months down the road for another PSA test and follow-up. I was a bit surprised that he wanted to wait six months, and suggested doing the test in three or four months. He was a bit insistent on the six month window. He felt comfortable with my current situation—the slight increase in my last PSA test from the previous one and my PSA doubling time—that waiting six months wouldn’t be a problem. He also argued that having a longer period between tests would better reflect what’s going on.
As we wrapped up, he reminded me that the scan results were good news, and I know that he’s right in that regard. I’ll work on changing my own perspective going forward (even though those little cancer bugs are still doing their thing inside me.)
My follow-up appointment is on 30 September 2025.
That’s it for today. Be well!
Header image: Cherry Blossoms, Japanese Friendship Garden, San Diego, California
You may have overachieved when your doctor asks, “Are you a urologist?”
I had a good meeting with the real urologist this morning, and it appears that he actually read the questions I sent to him in advance. That made the discussion easier.
First on my question list was whether a PSMA PET scan was warranted. He agreed that it was, and we’re going to try to get that scheduled soon. He thought that, with my PSA at 0.94 ng/mL, there would be a better chance of actually finding something this time. The only concern is that the VA has required a bone scan ahead of the PSMA PET scan in the past, and he’s going to see if we can skip that. It may take several days for the schedulers to call me.
We did discuss the possibility of further radiation if a lesion is found away from the pelvis. I mentioned that I had had blood in my stools and mild radiation proctitis discovered (and addressed) during my recent colonoscopy. He was not keen on further radiation to the pelvis under those circumstances. Neither am I.
My next question was about the timing of beginning androgen deprivation therapy (ADT). He was pretty squishy on the timing, not knowing exactly where we’re at. I mentioned that, a year ago, the urologist told me that we’d start when my PSA hit 2.0 ng/mL, but the medical oncologist suggested holding off until metastasis. He generally agreed with the concept of starting it later so that the cancer doesn’t become resistant to it prematurely, with one caveat.
He seemed to give more weight to my PSA doubling time than did other doctors, and that’s when he asked me if I was a urologist. I had presented him my graph showing my PSA progression, and it showed my PSA doubling time. “How did you know how to calculate it?” I told him that I used the Memorial Sloan-Kettering PSA doubling time calculator. To him, my PSADT of 9 months was creeping into “concerning” territory, and might make him a little more inclined to start ADT earlier.
I asked him, “At what point do we call this metastatic disease?” and, “When should we get a medical oncologist (MO) involved?” To the first, he said that all we know is prostate cancer is somewhere in my body, but wouldn’t go so far as to call it metastatic yet. To the second, he was open to brining in a MO if the results of the PSMA PET scan warranted it.
We agreed to the following plan:
Get a PSMA PET scan and meet again in six weeks to review the results.
Get an updated PSA test before the six week review.
Let the results of the scan determine if we get the MO involved at that point.
I have the six-week follow-up appointment scheduled for 1 April 2025. My concern is getting the PSMA PET scan scheduled and completed before then. If I need a bone scan in advance of it, that may complicate or delay the PSMA PET scheduling further. If push comes to shove, I already had an appointment scheduled with urology on 8 May 2025, so that’s not that much of a delay if we can’t get everything scheduled before 1 April. 2025.
It was a productive meeting from my perspective, without any surprises.
More to come as we get things scheduled.
Header image: Cuyamaca Rancho State Park, California
No surprise here. In my spreadsheet, I put a placeholder value of 0.50 ng/mL for this PSA test based on the previous trend, and the actual result came in slightly higher at 0.52 ng/mL.
It seems safe to say that the salvage radiation therapy failed to do the trick.
I am trying to describe my reaction to this hour-old news. I guess words that I might use would be: numb, indifferent, resigned. I don’t know. It’s a bit weird. I certainly had zero expectation that my PSA would go down or even hold steady given the previous trend.
You may recall the conversation with the medical oncologist suggested that we monitor and do another PSMA PET scan in six months, which would make it August. The question now is, based on these results, do we stick with that plan? Or do we move to the discussion on the type of androgen deprivation therapy and the timing of ADT?
I did ask the phlebotomist if he was drawing blood for a testosterone baseline test and he said yes. I don’t see the results posted online yet (my record is still going through its once-a-day update as I type this).
Well, it’s after midnight. I’ll sleep on this and perhaps I’ll be a tad more focused in the morning after having processed this.
What’s next:
9 May – Appointment with primary care physician (annual physical)
14 May – Appointment with urologist
Header Image: Scenes from San Diego Bay, San Diego, California
Is it just me, or is anyone else having pandemic days all blend together and you lose track of time? Late last night (technically very early this morning as I was tossing and turning in bed around 2 a.m.), I realized, “Crap! I didn’t even think about posting on my blog, let alone write anything!”
So here I am on my advertised posting day with three hours and one minute left to get this out on the 11th, and I pretty much have nothing. Well, that’s not entirely true…
I did come across this article on The “New” Prostate Cancer Infolink that talks about PSA doubling times with respect to prostate cancer progression in men with non-metastatic castration resistant prostate cancer.
Unfortunately, they weren’t able to access the full study report, and the summary that’s provided is pretty high-level, restating the obvious: Shorter PSADT is associated with shorter metastasis-free survival and shorter overall survival.
One of the things that I discovered working in a hospital is that I can sometimes access research reports like this via its computer network. I’ll see if I can access this report to learn more details about the study and, if I can, I’ll share anything I learn.
Whew! Finished with time to spare. 🙂
Stay well and keep living the pandemic life as best and as safely you can wherever you happen to be.
My last PSA test on 4 February showed a 50% drop in my value compared to the previous test in September 2019, which is a major, unexplained swing considering that I haven’t been doing treatments of any type to lower my PSA. It just didn’t sit right with me, so I asked for a retest.
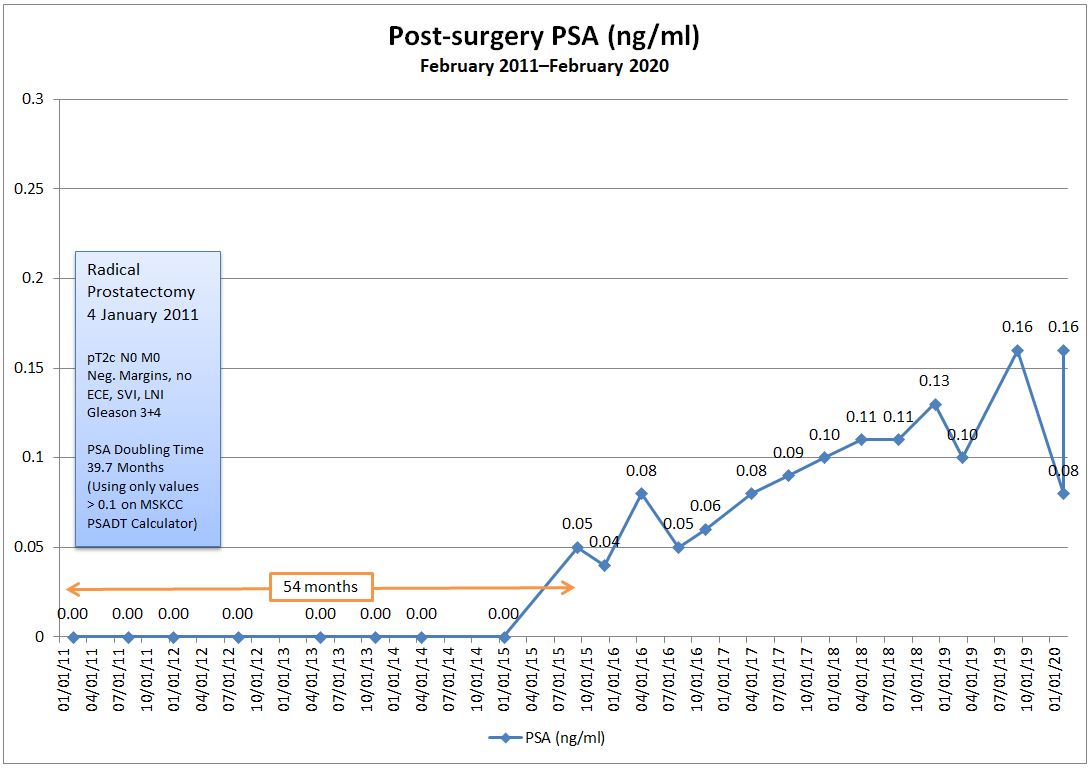
I went in on 20 February for the retest, and the PSA came back at 0.16 ng/ml, exactly where it was in September 2019. (At least that’s the silver lining in the cloud: it didn’t go even higher.)
We’ll probably never get a good explanation for the dip in my PSA earlier this month, and I guess that’s just part of dealing with this beast. I’m going to leave the errant data point on my chart just to show how wacky this can be at times.
The one thing that this has done, though, is drive my PSA Doubling Time down to 39.7 months according to the Memorial Sloan-Kettering PSADT Calculator (excluding the 0.08 reading). That’s still a very good number, but it’s downward trend over time is becoming more concerning.
I’m really glad that I was able to get the retest done before my appointment with the doctor on Tuesday. It certainly will make for an interesting discussion.