Baffled. Completely and utterly baffled.
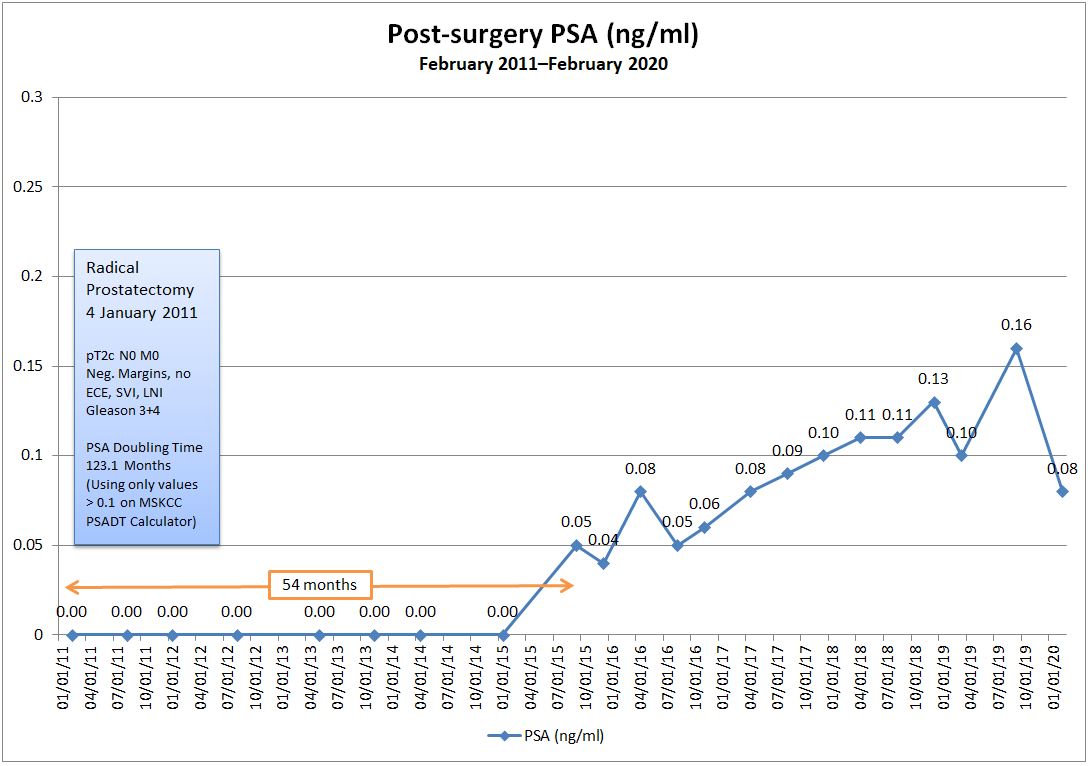
Excited that my PSA value went from 0.16 ng/ml in September to 0.08 ng/ml last week, but completely thrown for a loop as to how and why a 50% decrease happened (without any treatment or other intervention). The last time I was at 0.08 ng/ml was nearly three years ago in April 2017.
I follow the same routine for a week before each PSA blood test to avoid activities that may influence the outcome. The only difference time was that I had a cold/flu the days before the test (Monday afternoon-Thursday evening; blood draw on Friday morning), but I can’t imagine that having any influence on a PSA number. I’ll ask when I talk to the doctor on 25 February 2020.
I tried updating my PSA Doubling Time using the MSKCC PSADT calculator, and this bumped my PSADT from 43 months to 123 months. There is a caveat, though. The online calculator accepts only PSA values of 0.10 or more, so I rounded up my 0.08 to 0.10 to run the calculation.
I get that there can be lab errors or accuracy concerns as well, but I would be hard-pressed to attribute a 50% shift to a lab issue. Still, when you look at the last four data points on my chart, there is pretty significant fluctuation between each and its previous data point when compared to the quite consistent series of data points prior to that. It makes you go, “Hmm…”
Don’t get me wrong. I’m not complaining about where the PSA is at. I will say, however, that these kinds of wild swings make it challenging to wrap your head around what’s happening in order to prepare for what’s next. I was mentally gearing up for calls to imaging centers and radiation oncologists because I was expecting the result to be in the 0.16 to 0.18 range this time around.
So that’s it. A short post with unexpected, somewhat bizarre results. We’ll see what the doctor says on the 25th.