
To my regular readers, you may want to skip this post. This is a high-level update intended for my family and friends who don’t regularly follow this blog (gasp!), and it will be shared with them via my personal social media accounts. If you’re new here, welcome. Feel free to read away.
It’s been a while since I’ve provided any detailed update on what’s going on in the world of my prostate cancer, so here goes.
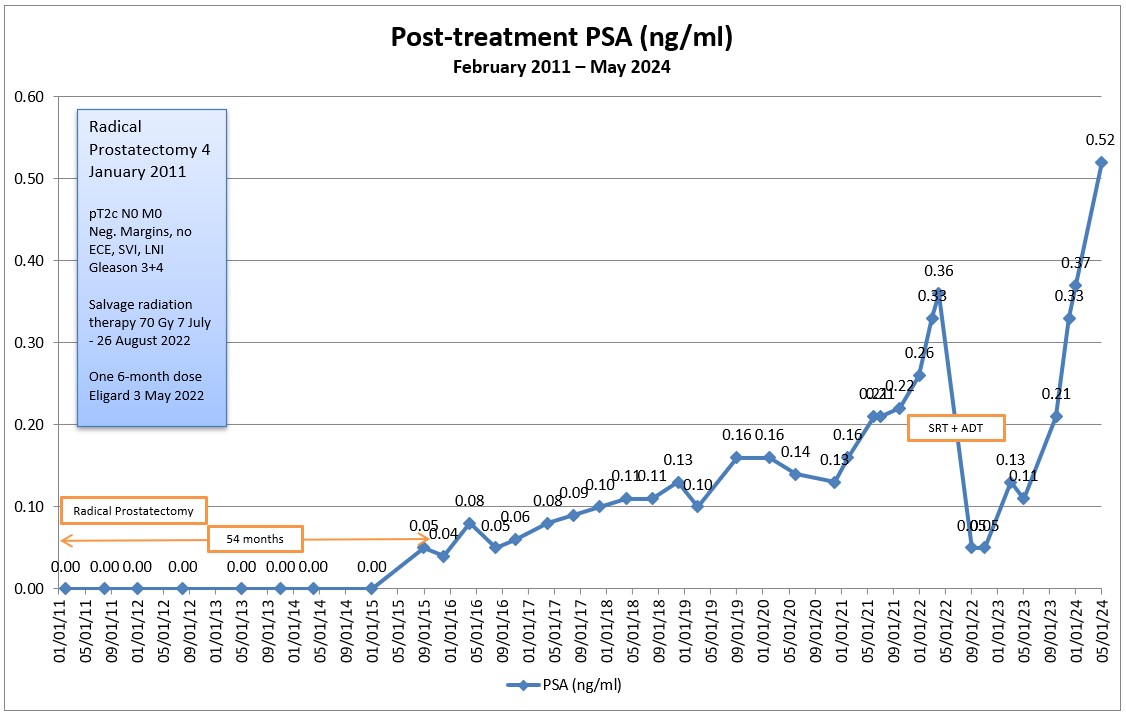
We last left our hero two years ago as he began 35 sessions of salvage radiation therapy on 7 July 2022 in attempt to kill off his recurrent prostate cancer after his surgery in January 2011 ultimately failed. Unfortunately, those little cancer cells have proved themselves to be quite resilient, and the salvage radiation therapy has failed, too. Bummer.
We know this by tracking my prostate-specific antigens (PSA) on a regular basis. After the surgery, my PSA level should have dropped to undetectable (zero) because there was no prostate left to produce the PSA. But the PSA can live on in the cancer cells even without a prostate, and that’s how we know the cancer is still there.
After the radiation, my PSA should have dropped substantially, and it did, at least initially. But about 15 months after the radiation ended, my PSA was on the rise again. It rose enough to the surpass the PSA level when we started the radiation. In May 2024, it continued its upward climb to 0.52 ng/mL, the highest it’s been since the surgery. (In the grand scheme of things, it’s still a low value that many fellow prostate cancer patients would love to have, but the fact that it’s doubling about every six months is a concern.)
There is a relatively new scan that can detect prostate cancer cells at fairly low PSA levels. It works best when the PSA is close to 1.0 ng/mL, but it has detected prostate cancer about 30% of the time at PSA levels in the 0.2–0.3 ng/mL range. I went for this PSMA PET scan in January when my PSA was 0.37 ng/mL, and the scan failed to detect anything.
On the one hand, that’s great because there were no signs of metastasis and no evidence of prostate cancer. But on the other hand, we need to know where the cancer is located and what it’s up to in order to plan our next treatment options. Because it didn’t reveal its ugly head, we can’t make any meaningful treatment decisions right now.
If there are one or two small lesions someplace, we may be able to radiate them again depending on their size and location. But if there aren’t any distinct lesions and my PSA continues to increase, that’s likely the result of micrometastases and that would require a systemic treatment approach (e.g., hormone therapy, immunotherapy, chemotherapy, or any combination thereof).
After reviewing my May PSA results with the urologist, we agreed to punt for six months and do another PSA test in late October. I know that seems counterintuitive—letting the cancer continue to grow without taking action—but there’s a reason for it. I’m predicting my PSA at that point will be in the 0.75–1.0 ng/mL range in October, and we’ll do another PSMA PET scan to see if we can determine what’s going on and then plan from there.
Up until this year, all of my conversations have been with the urologist and radiation oncologist. In February, I met with a medical oncologist for the first time because they’re the ones who deal with the systemic treatments.
Based on my conversations with the urologist and medical oncologist, the next logical treatment option is hormone therapy. Prostate cancer lives off of testosterone, so if we kill off the testosterone, we slow the growth of the cancer cells. (Hormone therapy is not curative, however.) But the timing of starting hormone therapy is important.
If we started the hormone therapy now, it would rapidly knock my PSA down so far that it would make it next to impossible to do the PSMA PET scan in November and get any meaningful results.
The other problem with starting hormone therapy too early is that the prostate cancer can become hormone resistant much in the same way that bacteria can become resistant to antibiotics. Start the treatment too early, and you’ll lose its effectiveness when you really need it later.
There seemed to be a differing of opinions between the urologist and the medical oncologist as to what would trigger the start of hormone therapy. The urologist would hold off until there’s evidence of metastasis; the medical oncologist suggested we’d start when my PSA hit 2.0 ng/mL. We can figure that out when the time comes, but both agreed that hormone therapy (and other therapies) can keep me around another 10–15 years (or more).
Of course, my quality of life may be diminished as a result of the treatments. Hormone therapy can come with a whole host of unpleasant side effects such as fatigue, muscle loss, weight gain, loss of libido, hot flashes, etc. No need to rush into that Disneyland of experiences.
Physically, I am feeling fine. I’m completely asymptomatic when it comes to the cancer, but the side effects from the surgery and radiation are present and are a nuisance more than anything. Psychologically, though, it’s been a bit of an emotional roller coaster ride as I go from PSA test to PSA test, and failed treatment option to failed treatment option. We’re closing in on 14 years since diagnosis, and it does get tiring.
One of my regular blog readers and my urologist both suggested that, at this point, I look at my prostate cancer more as a chronic illness than as a life-threatening disease. I’m still trying to embrace that perspective and, even if I do, the worry will never go away.
There you have it. The latest and greatest in this adventure of living with prostate cancer. Follow along if you want to see my monthly updates, and we’ll probably know more right around the holidays.
Be well!
Header image: Lake Michigan coastline from the John Hancock Center, Chicago, Illinois

Dan, thank you for sharing.
LikeLike
Thanks, Patrick! Hope all is well with you and your family.
LikeLike
Hi Dan, I am a regular reader but I appreciated the summary you put out on your blog.
Like so many with prostate cancer we have had similarities and differences. I still have a prostate because I was put on hormone therapy straight away as it was not confined to the prostate but imaging showed it had spread to my seminal vesicles. I have had 2 PSMA scans following treatments – chemo and hormone – and both lit up, on each occasion my PSA had risen to well over 2.0. The first showed a recurrence in the prostate itself but not to the abdominal lymph nodes. I then had radiotherapy to the prostate alone, my oncologist offered to radiate the prostate alone or the prostate and abdominal lymph nodes but since there was no indication from the PET scan of abdominal lymph node involvement I opted for radiotherapy of the prostate alone. Following my radiotherapy my PSA halved but did not drop to a low level and then started to rise again. The second PET scan which followed this revealed the prostate had been successfully radiated, still no involvement of the abdominal lymph nodes but the crafty cancer had jumped to lymph nodes in my chest area. Like you, I would not have been content to do nothing until there was traditional imaging proof of metastases which was the first option. However the PET scan evidence in my upper lymph nodes was enough for my oncologist to put me onto Enzalutamide and that was two and a half years ago. I have been and continue to be on Lupron ADT injections since 2017. My PSA dropped to undetectable very quickly and has remained there ever since. That will 3 years this November so I am delighted with the response.
You might like to see – or may already have seen – as I know you research everything carefully this publication in the New England Journal –https://www.nejm.org/doi/full/10.1056/NEJMoa2303974
I think you might be offered the choices between Lupron alone, Enzalutamide alone or Lupron AND Enzalutamide. You will see from the publication that Enzalutamide alone can give you almost as good a result as Lupron PLUS Enzalutamide. That’s a decision for you to make if I was in your shoes I might go for the Enzalutamide tablets alone to see what the response is like before considering the addition of Lupron injections if it was in any way disappointing on Enzalutamide alone. I hope your next scan reveals where the cancer is still active and that it is lymph nodes, which again is the most likely. The prognosis is as you say that you have well over 10 years ahead of you which compared with some is indeed fortunate. Please keep me posted on your progress via your dansjourney posts. And of course I wish you all the best. regards Charles (from Scotland).
LikeLike
Hi Charles,
Thanks for sharing your story and the article. It looked familiar to me, but worthy of a second look at it. In my initial discussion with the urologist and medical oncologist, they both were leaning toward starting with Lupron as a monotherapy. We’ll see where I’m at with my next PSA test in October/November and go from there.
All the best,
Dan
LikeLike
Dan, I’m a regular reader but I ignored your comment and read through it anyway. This note is a good overall view of what’s happened and where you are in the journey.
Please really try hard to as you said, embrace the perspective that this is indeed a chronic disease. Because for so many men, even the majority of men in a position such as yours, it really is just that.There have been so many advances in treatment over the years as I’m sure you know, and new studies are succeeding all the time. So take heart.
one more thing… I don’t know if you’ve heard of Dr Dean Ornish. He has done decades of research on Lifestyle Medicine and has shown that a program/lifestyle of diet (Whole Foods plant based vegan with no oils) along with daily exercise, stress management and support, can stop progression of, and even reverse Heart disease. The reason I mention this is, that he’s also done studies showing that the same program can slow or stop the progression of Prostate Cancer (and more recently, Alzheimer’s.) like I said, it’s hard. But ADT is no fun either.
This isn’t quack stuff. In fact after submitting his studies to Medicare, they now cover the $11000 (retail) cost of his 9 week program. Full disclosure: I’m on the program , trying to stop progression of heart disease, and in week 6. It’s hard. But I’ve seen amazing results in my numbers so far. you might want to look into it. And if you want more info, feel free to email me directly.
I wish you well, and hope any treatments you may need are far into the future.
sorry for the length of this comment.
LikeLike
Thanks for your comment, support and suggestion. I’m warming up to the chronic illness perspective over time.
All the best.
LikeLike
Great job Dan. It appears you are on top of things . I had the Prostate removed 3 years ago, then EBRT of 22 sessions and no ADT about a year go. The radiation of 22 sessions was for a slow rising PSA after surgery. So at 0.14 I got radiation. At first it didn’t do much , but now 1 year since radiation the PSA has gone down to 0.056 now , from 0.072 and 0.14 one year ago . Dr’s say that it will likely go down to zero from the current 0.056 , as it appears the cells were few and the radiation RAD’s were light , so it takes time. I have an anxiety issue with prostate cancer as my father passed away with prostate cancer about 28 years ago. I was his sole caregiver and he ultimately passed away with prostate cancer, which was a horrible death for him at that time. I was the one that pulled the sheets over his head when he passed away. Although it was 28 years ago, it still seems like yesterday. Hence, I have a terrible anxiety around prostate cancer. Before I was diagnosed three years ago, after my yearly physicals, I would go to the urologist to get a second opinion. Five years went by and there was no issues. On the sixth year the urologist said I had a rise in my PSA up to 4.0 and he would like to do a biopsy. At that point, he noticed 3+ for Gleeson in my prostate . I then did surgery , then EBRT 1 year later . I don’t have any symptoms, no bladder issues, and feel fine at this point. I am always haunted by the fear that the prostate cancer will come back, but I am in a very good spot right now with the PSA lowering drastically thank you for your articles and all your support. James on Vancouver Island . God Bless to all !
LikeLike
Hi James,
First, your comment landed in my spam folder here on WordPress, so my apologies for just seeing it now.
It’s great that the radiation seems to have taken hold and his keeping your PSA at bay. Let’s hope that it continues to do so for the long term.
I’m sorry about your father and can fully understand how that experience has shaped your views on prostate cancer. It makes perfect sense. But good on you for keeping on top of it knowing that there was family history. That’s really important for people to understand. In my case, there was no family history, so prostate cancer wasn’t on my radar.
Again, apologies for the delayed response and wishing you all the best,
Dan
LikeLike
Sent a reply …I think you got it .
LikeLiked by 1 person