No definite evidence of locally recurrent or metastatic disease within the abdomen or pelvis.
(If you don’t know, BLUF = Bottom Line Up Front).
There was one 9 mm kidney-shaped lymph node that caught their attention, but didn’t think it to be remarkable.
They also commented on a bunch of my other organs and bits and pieces, but nothing seemed too out of the ordinary for any of them aside from a few dents and scratches from 63+ years of normal wear-and-tear and countless miles/kilometers.
The fact that the CT scan didn’t pick anything of substance up is a good thing and a bad thing. Good because it didn’t see anything; bad because it didn’t see anything. The likelihood of it detecting the lesions at my PSA level were small, and we knew that going into this. So even though we didn’t see anything, that doesn’t necessarily mean that it’s not there.
I did get a chuckle out of one line in the report:
Multidetector CT abdomen/pelvis was obtained after the uneventful administration of intravenous contrast.
Uneventful for who??? The radiologist? Sure. I did everything in my power to not puke all over their $300,000 scanner. 😲
I expect we’ll have the same result with bone scan next week, but time will tell.
This morning, I went onto the UCLA website and filled out the form to request more information about the Ga68 PSMA PET scan and perhaps even schedule an appointment with them. We’ll see how long it takes for them to respond. I’m gue$$ing it may be pretty quickly as they want to get more people using their test and facility. Ju$t a hun¢h.
“Cynic, table for one. Cynic.”
That contrast used in the CT scan yesterday really kicked my butt. The juice was injected into me shortly after 2 p.m., and as I was heading to bed around 9 p.m., I could still feel some of the side effects from it.
I did drink a lot of liquids to help purge it from my system and that translated into multiple runs to the toilet through the night last night. Oh well. It all caught up with me around 2 p.m. this afternoon when my ability to focus just ran head-on into a brick wall. I hung it up at the office and came home.
I just checked for the scan results online, and nothing posted yet. I suspect it will be on the weekend that I’ll be able to see them. Of course, they’re usually written in such a away that a lay person has trouble comprehending what’s on the page. We’ll give it a try, though, when the time comes.
That’s about it for today. Hopefully, the next post has news about the PSMA test or the CT scan results, or both.
You know me. I love tracking things, and this post is the 400th published post on this blog. Woo-hoo! 🎈🎉✨ Of course, I would have preferred to not have written any of them at all, but that’s life.
I thought I had had a CT scan in the past, but if I did, I don’t remember it being anything like what I experienced today. It kicked my ass. Technically, it was the contrast they injected into me that kicked my ass. The scan—sliding in and out of the scanner—was a non-event.
The radiologist forewarned me of the sensations that I would experience shortly after he injected the contrast. The sensation of a full and warm bladder? Check. Metallic taste in my mouth? Check. A warm sensation throughout my body? Check.
What he didn’t do a very good job of was forewarning me of the intensity of the some of these things. At one point, I thought I was going to vomit like Vesuvius. It was awful. As soon as he stopped the IV flow of contrast, I could feel some of these side effects dissipating. (But not nearly as quickly as they came on.)
I didn’t even bother to ask the technician if they saw anything odd on the scan as they were running the test. I’ll usually do that because sometimes, if you’re lucky, the technician will help you out. They may not be able to be all that specific, but I’ve had one or two tell me, “You really don’t have anything to worry about.” I was just more focused on getting out of there without puking.
The whole appointment went like clockwork and went faster than I expected. My appointment was for 2:30 p.m. I pulled into the parking garage at 1:45 p.m.; was checked in a Radiology by 2 p.m.; on the scanner bed by 2:10 p.m.; and headed back to my car by 2:35 p.m. Again, I know there are tons of complaints about the VA healthcare system, but San Diego VA Medical Center has been top-notch as far as I’m concerned.
The radiologist thought they would have the full results available by Friday.
I’ll have to admit that on my commute to work this morning, I had a bit of a knot in my stomach. Not because I was afraid of the scan (now I am—a little), but because this is the beginning of the process that will give me results I may not want to hear.
On a related note, my employer-provided healthcare insurance did confirm that the Department of Nuclear Medicine at UCLA is in network, so that’s a good thing.
What’s next? Here’s an estimated timeline:
Get online access to CT Scan results sometime this weekend or early next week.
Have the bone scan on Friday, 23 July.
Get online access to bone scan results 3-5 business days after the scan.
Have a follow-up appointment to review both scan results with the urologist on 3 August.
I’ll contact UCLA to start that process and hopefully have all of my homework done in time for the appointment on 3 August.
Well, time to drink a few liters of water to purge that contrast out of me.
Anticipation for this appointment really did a number on me for some reason. I was nervous to the point of feeling queasy as I was driving to the San Diego VA Medical Center, which is quite unusual given how many times I’ve done this. I guess that this was different because my PSA had broached that dreaded 0.2 ng/mL mark.
Okay. I started this post (above) while sitting in the waiting area waiting for my appointment, and afterwards, my plan was to sit down at home this evening and summarize what we discussed. But the doctor just called a few minutes ago with some information that completely changes how I’m going to approach this post.
PSA Results
In a nutshell, one of the things we discussed was re-running the PSA test to see if last month’s 0.21 ng/mL was a real reading, or if it was an anomaly like the February 2020 drop from 0.16 ng/mL to 0.08 ng/mL. She even asked me if I had had an orgasm or rode a bicycle or did other similar activities before the June test. I had done none of those.
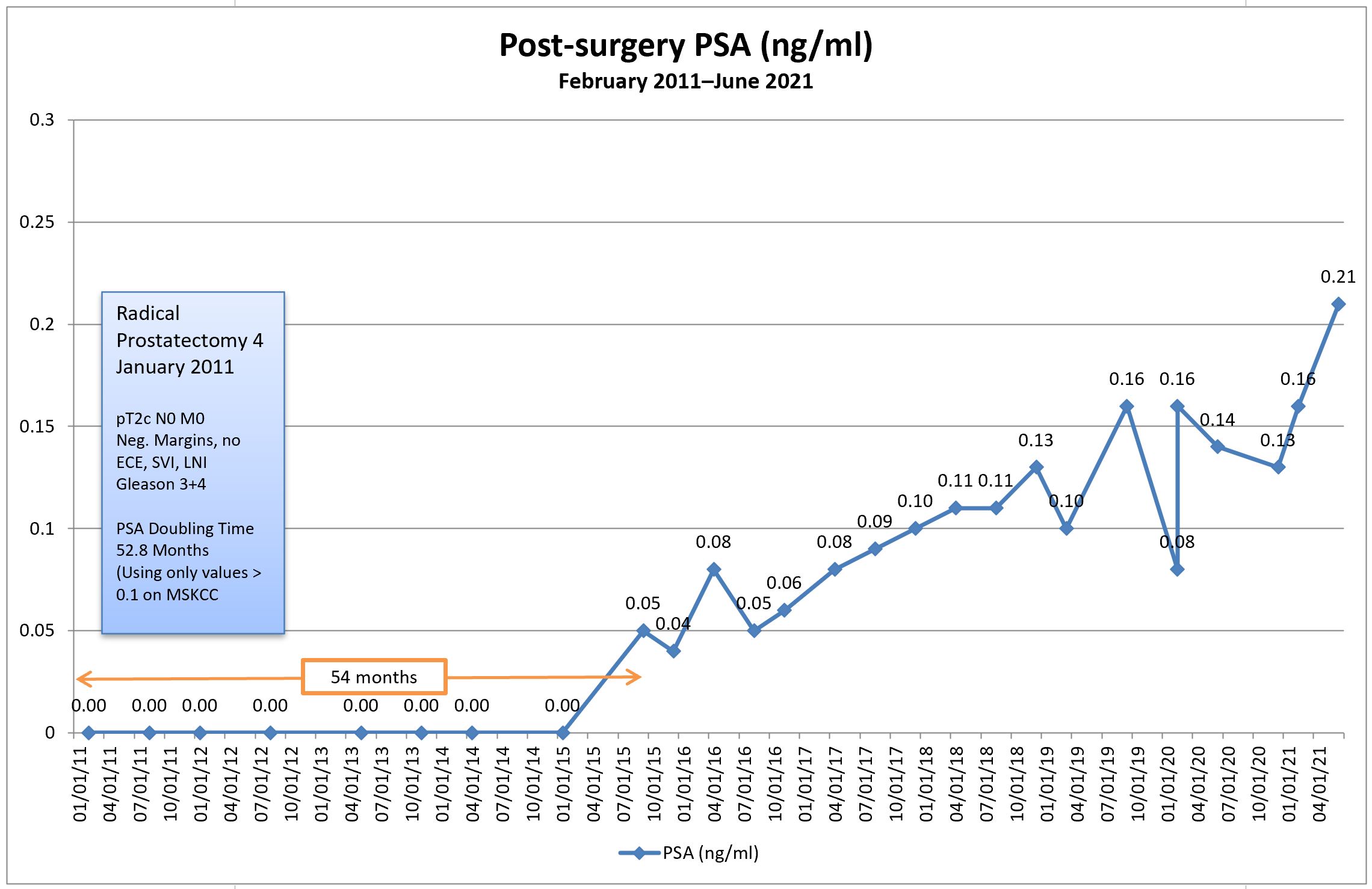
I asked to have the test re-run for peace of mind and she put the order in the system. She said that she should be able to see the results later this afternoon before they’re posted online, and instructed me to call her later in the day. She just returned my call with the results: my PSA came in at 0.21 again, confirming the June result. (You can also see that my PSA doubling time dropped to 48.1 months from 52.8 months in June.)
Note the addition of PSA doubling time to the chart in red, showing the PSA doubling time in months (right axis). [Click chart to enlarge.]
I’m not pleased that I’m hanging out in the 0.21 range, but I am pleased to have the confirmation. Now we know what we’re dealing with.
Plan A
During the consultation, we talked about possible courses of action. The first was to get the results and, if they were still hanging in the 0.16-0.18 range, we’d continue to monitor, perhaps bumping the frequency of PSA tests to three or four months instead. Obviously, that plan got tossed out the window.
Plan B
If the PSA came back with a confirmatory value, we agreed that scans to try to locate the cancer would be an appropriate next step. That was a great opening for me to talk about the Ga-68 PSMA PET scans at UCLA, but more on that later.
One thing that I’ve noticed in my years of being cared for at the VA Medical Center is that they do seem to be a tad slower to embrace some of the new technologies, definitions, and treatment options that are out there. Their protocol for someone in my situation is a bone scan in combination with a CT scan, so that’s what I’ll be calling to arrange tomorrow.
I argued that it’s very unlikely that the bone scan will pick up anything at my PSA level, and my doctor’s response was that we might be surprised. Ditto for the CT scan. If both scans are negative, the protocols would allow us to proceed to an Axumin PET scan done at the VA Medical Center. If the Axumin PET scan came back negative, then we may be able to figure out a way to get the PSMA PET scan at UCLA.
Of course, my preference would be to go straight to UCLA and skip the bone, CT, and Axumin scans altogether, but if those are the protocols that may get me answers I’m seeking, then I guess I need to follow them. Even so, I may try to push for the PSMA PET in place of the Axumin (I even mentioned to her that I may be willing to pay for it myself if the VA and my own insurance didn’t cover it).
General Conversation
One of the questions that I asked was about when the actual PSA value trumps the PSA doubling time when it comes to deciding to take action. Clearly, each case is unique and there is no definitive answer, but my doctor’s take on it was that she wouldn’t let a PSA go above 1.0 ng/mL without taking some action.
She did, however, bring up the fact that it’s becoming more widely accepted to do exactly what I’ve been doing—continuous monitoring. Too many patients are being overtreated with salvage radiation therapy with no guarantee of it being curative. She referenced how the American Urological Association (AUA) and National Comprehensive Cancer Network (NCCN) guidelines have been evolving over the years in a way that supports monitoring over action in some cases.
When I brought up the Ga-68 PSMA PET scan, it seemed that I may have been a little more up to speed on the topic than she was. We talked about it being FDA approved at UCLA and she reminded me that, just because it’s approved doesn’t mean it’s covered under the VA or private insurance yet. I agreed, and that’s when I mentioned I may be willing to pay for it myself.
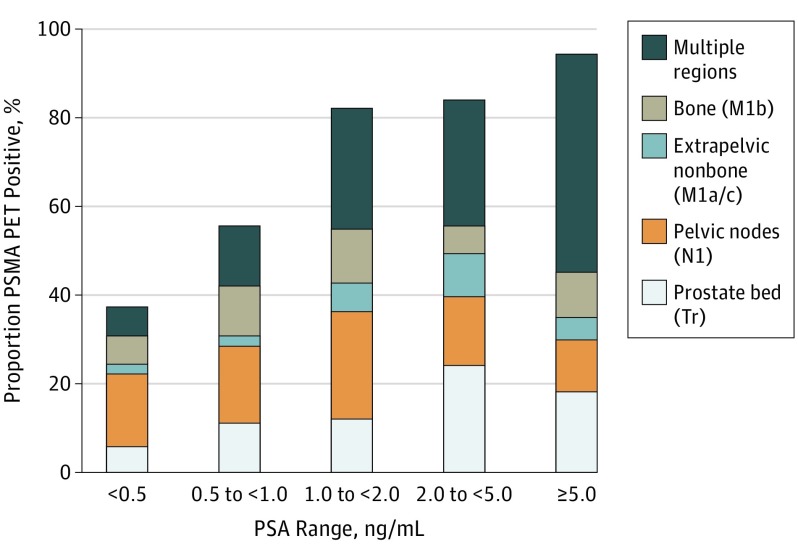
I brought a hard-copy of this paper on the Ga-68 PSMA PET scan and left it with her for her review. We also reviewed the chart showing what the scan was picking up at various PSA levels, and where it was picking it up.
I found it interesting that one of the first things she looked at with the paper was who the authors were. I guess quacks write papers, too.
Final Thoughts
It’s been one helluva weird day, that’s for certain. It started with me feeling uncertain and queasy and, in a bizarre twist, I feel as though I’m ending it on a high note.
Sure. No one wants to have recurrent cancer. It sucks. But now I feel the uncertainty brought on by PSA results bouncing around for the last six years is finally coming to a close, and I can really begin to focus on what happens next. There’s a sense of direction, albeit down a path none of us would like to go down. (Yes, there’s lots more uncertainty ahead, I’m sure, but I’ll cross that bridge when I get to it.)
Tomorrow I’ll call to get the bone and CT scans set up and, once we know the dates, I can arrange a follow-up appointment to review the results.
If they come back negative, then we try the Axumin or PSMA PET scan if possible. Of course, I’ll be doing some reading on Axumin scans in the interim (I really haven’t focused that much on them as an option, so I need to learn more about them).
Having cancer sucks. Having more definitive information doesn’t.
I came across this video highlighting Ga68 PSMA PET imaging from the doctor at the University of California San Francisco who helped with developing this imaging technique. It’s a bit long and a bit technical in some places, but gives a good overview.
I went for my originally scheduled six-month PSA test last Thursday and was able to look online last night to see the disconcerting results: A substantial increase to 0.21 ng/ml.
Breaking the 0.2 ng/ml threshold now officially puts me into the biochemical recurrence category, at least according to the long-held definition of biochemical recurrence.
Needless to say, I felt gut-punched on seeing the results. Sure, I’ve know for over five years that my trend has been upward, but I guess I got comfortable with it bouncing around the 0.10 to 0.16 range for the last few years. I wasn’t expecting such a substantial leap between my “surprise” PSA test in February and this one in June.
When it comes to PSA doubling time, it dropped from 67.7 months to 52.8 months with this latest test result included in the calculations. If I look at only the five most recent test results, the PSA doubling time drops to 46.5 months. Of course, all of those are great numbers that a lot of guys would like to have.
My appointment with the doctor isn’t until 6 July, and it will be an interesting conversation now that we’ve crossed that magical line of 0.2 ng/ml. In a way, I’m glad I’ve got several weeks to think this through and to come up with good questions to ask so that I’m prepared for the appointment.
Of course, salvage radiation therapy just moved to the top of the list of things to talk about. It will be interesting to see if their recommendation changes given the 0.21 number versus the long PSA doubling time.
Needless to say, there’s going to be much reflection and research in the weeks ahead.
Well, I missed last month’s post and this month’s is late. You would think that with all the quarantine time on my hands, I would have been a writing fool. Not so.
I did come across this study a while back that talks about PSA coming back after surgery and whether it’s wise to treat or watch.
My interpretation of the paper with my specific numbers kind of reinforces what the doctor told me at my last visit: that I’m okay continuing to watch my PSA for now. Others with different numbers may come to a different conclusion. We’re all unique, after all.
I’m scheduled for my next follow-up with the doctor the first week of July, so I’ll have to get my blood drawn for the PSA test in late June, assuming the COVID restrictions are lifted by then.
You may recall my last post where I talked about taking medication to lessen the nerve pain in my leg. I started the medication on 30 March 2020 and I seemed to hit the side effects jackpot. They knocked me for a loop, at least initially (hence, no writing).
Headaches, dry mouth, nausea, diarrhea, and extreme fatigue plagued me the first two weeks, but the good news was that the nerve pain was reduced a good 50% to 70%. The side effects were so troubling in the first few weeks that, by the middle of the third week, I cut the dose in half, but the nerve pain returned.
I’m back on the full dose now, and my body seems to have adapted to a degree. The fatigue is still present, the dry mouth is still there, and the nausea is very mild and only early in the morning. (No, I’m not pregnant.) The pendulum swung in the complete opposite direction on my GI system–constipation is now the norm. Sorry. I’m oversharing once again.
We did discuss physical therapy as part of my treatment plan, but that was just as COVID was rearing its head, so that’s been put on hold for now.
I had been fortunate enough to be able to work from home since 16 March because of COVID-19, but I’ve returned to work in the office at the hospital beginning last week.
On the whole, I’m pretty comfortable being in the office again. Sure, there’s a more risk than just sitting at home, but my office is well away from a high-traffic area of the hospital and I’m literally the only person here. I don’t have to go into any of the wards, and the walk from my office to the exit is relatively short. I probably feel more at risk in the grocery store.
California was one of the first states to impose a stay-at-home order and we’re being very cautious and deliberate in our re-opening. Some will say that we’re being too slow, but not me. Our efforts really did make an impact on controlling the virus. We’ve got nearly 40 million people in the state and we have just over 80,000 positive cases and 3,240 deaths. Contrast that with New York state with 19.5 million residents with over 351,000 positive cases and 28,339 deaths.
No matter how you slice it, though, it’s universally tragic. We’re all anxious to get this under control and behind us.
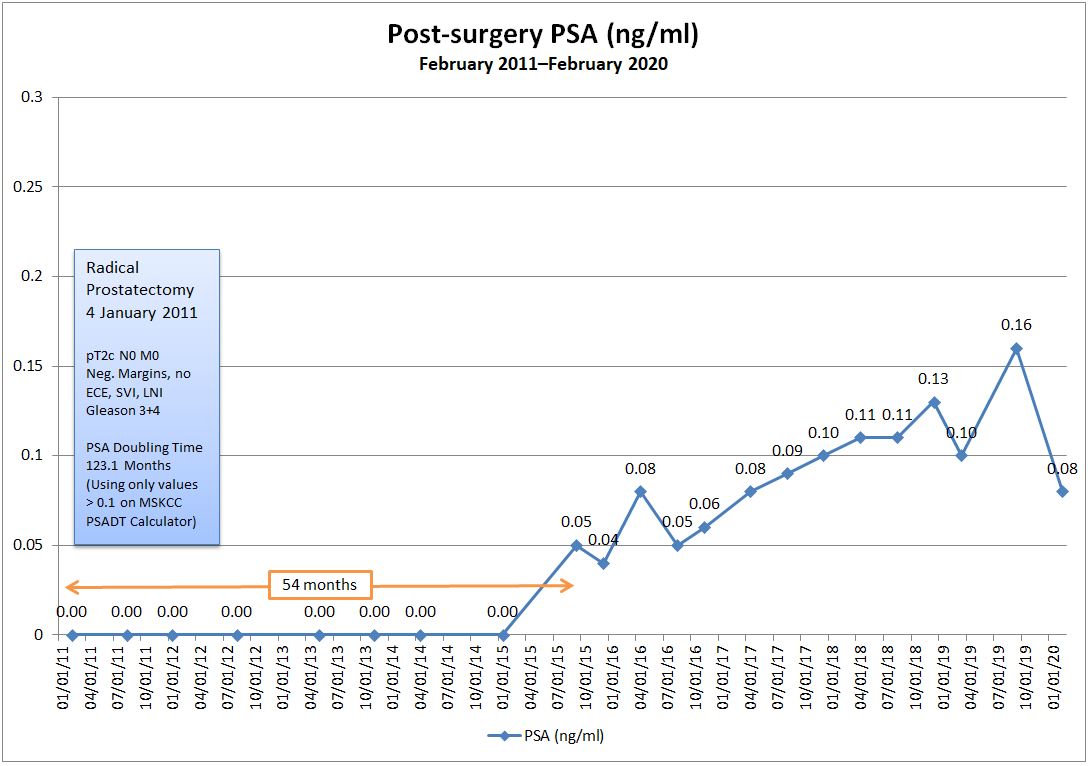
Excited that my PSA value went from 0.16 ng/ml in September to 0.08 ng/ml last week, but completely thrown for a loop as to how and why a 50% decrease happened (without any treatment or other intervention). The last time I was at 0.08 ng/ml was nearly three years ago in April 2017.
I follow the same routine for a week before each PSA blood test to avoid activities that may influence the outcome. The only difference time was that I had a cold/flu the days before the test (Monday afternoon-Thursday evening; blood draw on Friday morning), but I can’t imagine that having any influence on a PSA number. I’ll ask when I talk to the doctor on 25 February 2020.
I tried updating my PSA Doubling Time using the MSKCC PSADT calculator, and this bumped my PSADT from 43 months to 123 months. There is a caveat, though. The online calculator accepts only PSA values of 0.10 or more, so I rounded up my 0.08 to 0.10 to run the calculation.
I get that there can be lab errors or accuracy concerns as well, but I would be hard-pressed to attribute a 50% shift to a lab issue. Still, when you look at the last four data points on my chart, there is pretty significant fluctuation between each and its previous data point when compared to the quite consistent series of data points prior to that. It makes you go, “Hmm…”
Don’t get me wrong. I’m not complaining about where the PSA is at. I will say, however, that these kinds of wild swings make it challenging to wrap your head around what’s happening in order to prepare for what’s next. I was mentally gearing up for calls to imaging centers and radiation oncologists because I was expecting the result to be in the 0.16 to 0.18 range this time around.
So that’s it. A short post with unexpected, somewhat bizarre results. We’ll see what the doctor says on the 25th.
Tuesday’s meeting with the urologist was a bit anticlimactic. In a nutshell, we’re returning to the four-month test cycle and we’ll see what the next test will bring in late January or early February before we do anything.
The doctor had no explanation for the swings in my PSA level from 0.13 to 0.10 to 0.16 and reminded me that there could be a margin of error on the readings. (But he couldn’t quantify what that +/- error might be using the assay that they’re using.) He mentioned that riding a bike, other mild “trauma” to the pelvic region, or sexual activity before a PSA test could affect the results. That’s something that I already knew, so I make it a point to avoid any of that for at least a week before the blood sample is drawn to avoid introducing that variable to the picture.
He also reminded me that the historical definition of biochemical recurrence has been 0.20 ng/ml and suggested that it was premature to start thinking about salvage radiation therapy. Even so, he acknowledged that my PSA is definitely trending upward and worthy of continued monitoring so that it “doesn’t get away from us.” He suggested it would be fine to retest in six months; I opted for four.
One of the reasons that he was so comfortable with a longer test cycle and continued monitoring was my lengthy PSA doubling time. He also talked about the possibility that this could be residual benign prostate tissue left behind after the surgery that could be causing the PSA to increase again.
I filled him in on the Ga-68 PSMA PET/CT scan trial going on at UCLA and the option to shell out $2,800 to have the scan done outside of the trial. We talked a little about the successful detection rates at my PSA levels, to which he replied, “You know more about it than I do.”
We also spoke briefly about the potential long-term side effects of salvage radiation therapy, as well as the success rates of having no evidence of disease five years later. Nothing new was learned there.
On the whole, I’m generally on board with this approach—for now. But I will say that, mentally, I prepared myself for the meeting to go in a different direction, so I’m still processing that. If I’m perfectly honest, I’m a teeny bit less confident that waiting another four months is appropriate.
It’s as though I’m taking another step on a tight rope with each successive PSA test. The further out I go, the more the rope sways and it’s just a question of how long I can maintain my balance. Can I make it all the way across, or will I lose my balance and tumble into the abyss of metastasis?
Sure, I can opt to use my emergency safety harness—salvage radiation therapy—at any time, but that comes with costs potentially impacting quality of life: increased incontinence, loss of sexual function, scarring from radiation, etc. And—guess what?—at the end of it, I’ll be back on another tightrope taking another step every 3-6 months with new tests to monitor the effectiveness of salvage radiation. (And there’s a 30%-70% chance that I’ll fall off that tight rope into the abyss, too, depending on which study you look at.)
The trick is knowing when to decide whether you should keep walking on the original tight rope or that it’s time to jump into the safety harness. That decision is complicated by your coaches on the ground yelling conflicting things at you. Coach Radiation Oncologist is yelling, “Use the harness!” and Coach Urologist is yelling, “Keep walking!” Your own mind, filled with reliable information you gathered from Dr. Google, is adding to the confusion. It can be maddening to try and sort through it all and make the best decision possible.
That thought led to the last point of discussion with the urologist on Tuesday. He acknowledged that the field of prostate cancer research is a very dynamic one, and that there’s often conflicting guidance as new therapies are being tested and new discoveries are made. He also reinforced that prostate cancer is an insidious disease in how it behaves and how challenging it can be to treat it.
Prostate cancer is not an “easy cancer.” Far from it.