
I met with my doctor this afternoon to review my increasing PSA results, and it went just about as expected. There’s increasing concern, but things are progressing slowly enough that we can continue on the four month test cycle for now. That means I’ll be doing this all over again in April.
There were a few reality check moments in the conversation, though. I’ll get to those in a moment.
One thing I need to learn to do is shut up—at least for the first part of the meeting with the doctor. I’m not very good at letting the doctor talk and offer up his thoughts and recommendations and then ask the questions that I have. I just launch into a barrage of questions based on the research that I’ve done and assault the poor guy. On a positive note, he really didn’t dispute anything that I told him nor did he tell me that I was completely out to lunch on certain issues.
We reviewed the success rate for SRT, with various studies showing it to be 35%-55% effective at being progression-free at 5 or 6 years. (Here’s one.) We also discussed the potential side effects of SRT, and he did seem to believe that the risks were lower than I thought they may be.
The conundrum of starting SRT early versus knowing where to radiate based on imaging came up as well. My sense was that he’d prefer to start SRT while the PSA is less that 0.2 ng/ml, and certainly before it reaches 0.5 ng/ml, assuming that the cancer remained in the prostate bed. Doing so, he said, offers the best chance for success. He suggested that, if we wait until it would be detectable on even the most sensitive imaging (which can’t detect anything reliably until the PSA hits the 1.5-2.0 range), that radiation would do little if any good at that point, as the cancer will likely have spread. Androgen deprivation therapy (ADT) would be the treatment option of choice at that point, and ADT is not curative. It only prolongs life (with substantial side effects impacting quality of life).
The reality check moment for me came with his comment about waiting too long to the point where SRT wouldn’t be effective, and that ADT would be my primary treatment option. That really was an, “Oh, shit,” moment for me. It’s very easy to sit here and speculate how I will act in hypotheticals, but at some point in the future, I am going to have to make real world decisions that affect my longevity and quality of life.
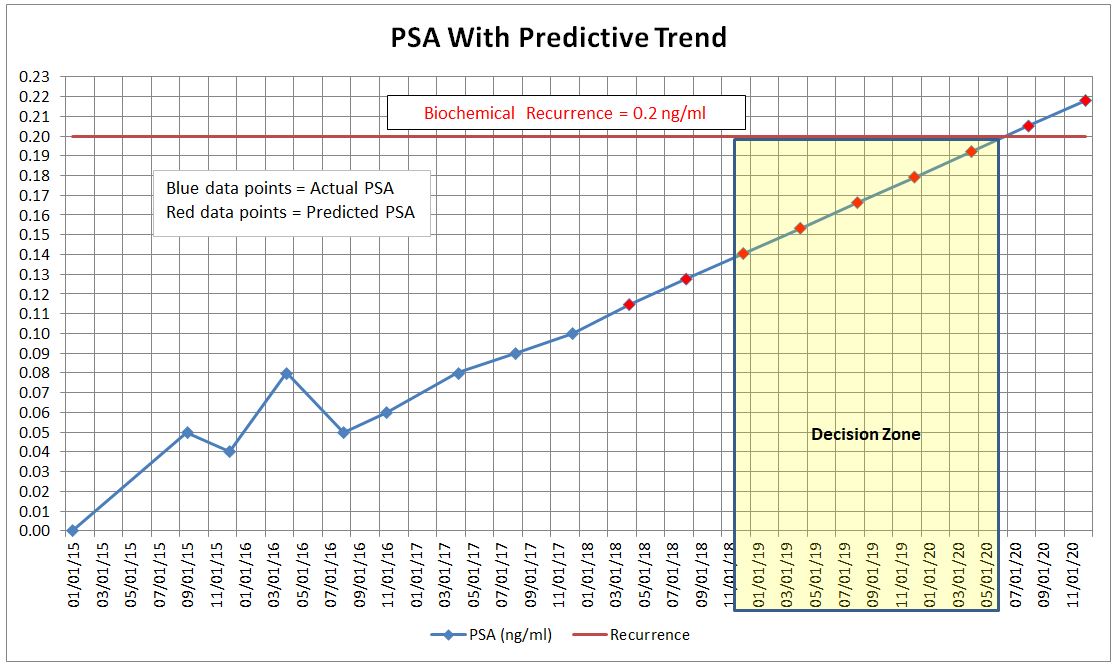
Based on my slow PSA doubling time (around 16 months), if my PSA progresses at its current rate, I’ll have 12 to 28 months to think about this and make my decision, based on whether I want to act if my PSA is around 0.15 or let it go all the way to 0.20. (See my “decision zone” in yellow below—yes, I had to geek out in my spreadsheet once again.) If I want to wait until it’s all the way to 0.5, I’ll have even more time.
Of course, one option is to do nothing. A study in 1999 showed that it took, on average, 8 years after PSA levels began to rise to reach metastasis, and another 5 years after metastasis to death.
The bottom line is that this is becoming increasingly real and that there will be some tough decisions in the next year or two. Of course, those decisions are mine and mine alone, and will be based on a variety of factors, not least of which will be my risk tolerance and any treatment’s impact to quality of life.
On that happy note, I wish you a Merry Christmas and a happy 2018! 🙂
Thanks, too, to those who took time to answer my questions in my salvage radiation therapy survey a few weeks ago. Your insights were quite helpful to me.

Thanks Dan, Merry Christmas and may you be at peace with all your decisions. It’s a tough road to trudge. I look to you for inspiration, for all of us who must make those decisions.
LikeLike
Thanks, Sean. The good thing is that I have a bit of time to make any decisions given how slowly my PSA is rising.
LikeLike
Dan,
There is a clinical trial currently ongoing on a new type of PET scan that shows promise in locations the site of recurrence. Might be better than choline or f18. I couldn’t find it but can call someone for the info if you are interested. You wouldn’t be eligible now, but would once PSA hits .2
LikeLike
Hi Ken. Thanks for the offer about the clinical trial–it would be interesting to learn more about it. I just came across a paper about PSMA PET scans in the December 2017 Journal of Nuclear Medicine. I need to re-read it to make sure I understand it correctly, but it, too, looks like a step forward.
LikeLike
Have a Merry Christmas!
LikeLike
Thanks, Andrew! Same to you and your family.
LikeLike
Thank your post. Have a Merry Christmas!
LikeLike
Dan, it is great that you have been so honest with your blogs all the way through your journey. It is want newbies (3 months after op) like me need.
Stay positive mate.
Happy new year
Clive
LikeLike