My visit to the urologist this afternoon went just as expected, and even a little better.
With the San Diego VA Medical Center being a teaching hospital, it’s rare that I see the same doctor twice. Because I liked the doctor I saw last time because of the conversation we had and the plan that we mapped out together, I specifically requested to see her again this time. Unfortunately, a young resident showed up in her place.
That actually may have worked to my advantage.
Dr. K started the conversation by asking if I had come to a decision as to whether I wanted to do salvage radiation therapy or hormone therapy. I was a bit taken aback by that—”Haven’t we skipped a few steps here, Doc?”—but then I remembered the way that Dr. L wrote up her notes from my visit with her, it would be easy for him to come to that conclusion.
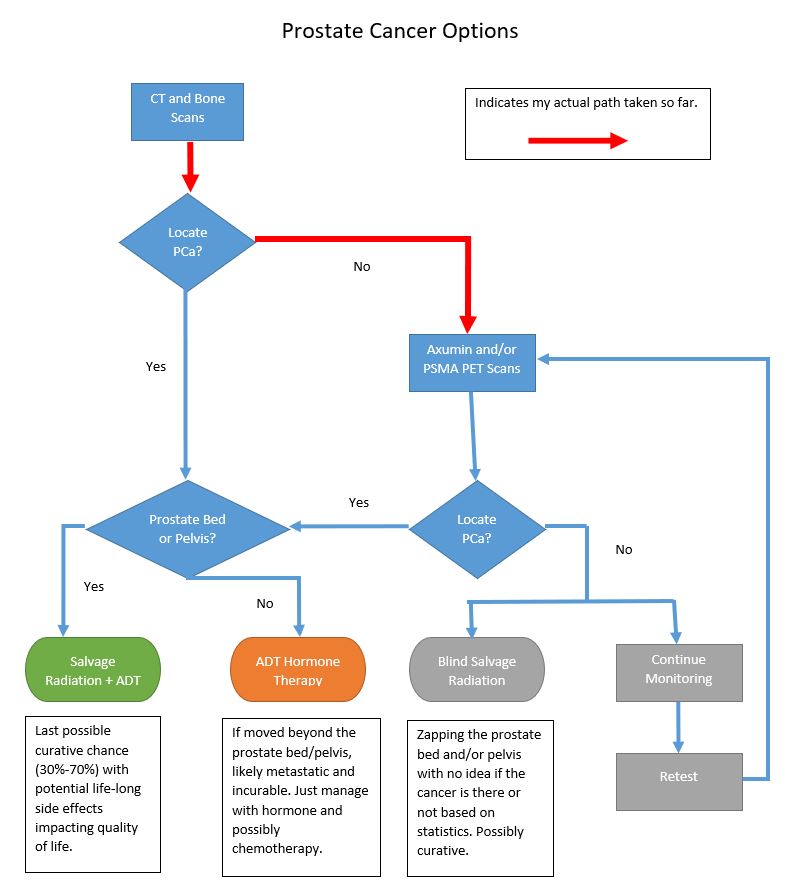
I filled in a few of the blanks with Dr. K regarding our plan to follow up the negative CT and bone scans with an Axumin or PSMA PET scan in hopes of finding the cancer before making the SRT vs. ADT decision. He dutifully reminded me that either or both scans could come back negative, too, meaning that the cancer was still likely in the pelvis or prostate bed.
Interestingly, when we were talking about the merits of the Axumin and PSMA PET scans, he immediately went to, “Why even bother with the Axumin scan; go straight to the PSMA scan.” I didn’t even have to nudge him in that direction. He and I were on the same page.
To his knowledge, though, SD VAMC had not yet referred anyone to get a PSMA PET scan, but he seemed eager to figure our how to make it happen and have me be the first (or among the first) to be referred. He wasn’t even sure where to begin, so I told him.

I opened my file folder that I had with me and pulled out the one-page sheet that I had put together, stepping him through the referral process that UCLA had shared with me. It was all there for him, and he asked, “May I keep this?”
He did admit, though, that he had no idea how long it may take to get approval from the hospital team before he could even ask for the referral, so this may play out over a few weeks or longer. Rest assured that I’ll keep on top of this, asking for periodic updates.
I’m pretty excited that we’re moving in the direction of going straight to the PSMA PET scan, but also recognize there can be a number of administrative twists and turns along the way.
In the interim, we agreed to test my PSA again in early November, keeping on a four-month testing cycle. I’m okay with that while we’re trying to sort everything else out.
We also talked about my incontinence episodes becoming more frequent and more substantial in the last 6 weeks or so. He wanted to rule out a urinary tract infection, so he sent me off for some labs and we’ll see what they yield.
These episodes have put me back in incontinence pads for the last few weeks. Before, a sneeze or a cough would yield a few drops; now, they yield a squirt. Not good.
More to monitor and report on going forward.
That’s it for this post.
Be well!