Before getting into the conversation with the urologist, I went for my bone density scan last week. The results? I have bones. They’re dense (i.e., normal). Now we have a baseline for future reference for if and when I start down the hormone therapy path.
Yesterday’s meeting with the urologist was unusually animated, if not bordering on contentious. The appointment was late in the afternoon (around 3:45 p.m. when she arrived), so perhaps she had had a crappy day and was ready for it to end.
I tried explaining my conversations with both oncologists, and she kept interrupting, sometimes with questions that made it seem that she wasn’t paying much attention. (She was on her computer reviewing my file as I talked; usually she’ll have reviewed the file before even walking into the exam room.)
At one point she said, “You have three cooks in the kitchen and should probably stick with one,” referring to the fact that I had two oncologists and her trying to manage my case.
When it comes to treatment, she’s still of the opinion to wait until metastasis to start hormone therapy, mainly because of the associated side effects and possible earlier resistance to the therapy. I mentioned that both oncologists recommended intermittent hormone therapy, and she seemed puzzled by that for some unknown reason.
I mentioned that the plan was for me to have another PSA test in the first week of September and, if warranted, a CT scan and bone scan in December. She seemed indifferent and offered no comment one way or the other.
By the end of the appointment, it was pretty clear that she was of the mindset that there’s little that she as a urologist can do at this point in my case management, and that the ball belongs squarely in the court of the oncologists. I agree. She did say, though, that if I start to have urinary symptoms that may be from the radiation or surgery (e.g., strictures, worsening incontinence), to come back to Urology for investigation and possible treatment. We did not set up a follow-up appointment for Urology.
Back in April, the oncologist suggested they take the lead on my case and, after yesterday’s appointment with the urologist, it’s clear that that’s what needs to happen.
I’ve got the PSA test on my calendar on 2 September. We’ll get the results, calculate PSA doubling time, and consult with the oncologists to determine the next steps based on the results.
If my PSA shoots up again like it did between December and March, reducing my PSA DT, I might be more inclined to act. But if it continues on a flatter trend like it did between March and May, I’d be inclined to kick the can down the road another three months.
So I’ll continue to live life in three-month increments until the results tell me it’s time to do something. Good thing I have a lot of hurry-up-and-wait experience from the Navy. 🙂
My visits with the medical oncologists yesterday and today went well, and there was some consensus on how to proceed.
[BLUF: We’re kicking the can down the road three months.]
UCSD Oncologist
The first part of the meeting was getting the doctor up to speed on my case, as he didn’t have any of the history. Of course, nerd me came prepared with a two-page Reader’s Digest chronological summary of my diagnosis and treatment, printouts of my PSA charts, and copies of the PSA doubling time (PSA DT) calculations.
PSA Doubling Time
Because PSA DT is an important number in the decision-making process, I opened the conversation by asking him how many data points should be used in the calculations. He chuckled a bit before saying that one of the downfalls of using PSA DT is you can pick and choose the data that you want to get the answer that you want. So true.
I calculated my PSA DT using 3, 4, and 5 values and came up with different answers:
Number of values used
Going back X months
Calculated PSA DT
3
6
7.6 months
4
9
8.0 months
5
14
9.2 months
He just looked at the curve on my PSA tracking chart and estimated in his head that it was around nine months. In his eyes, that six to nine month PSA DT warrants closer observation and monitoring.
Inconclusive PSMA PET scans
We discussed my four inconclusive PSMA PET scans and [F18] FDG PET scan, and whether he thought that I was PSMA negative. He thought it was unlikely that I was, offering up a case with another patient whose PSA was over 50 ng/mL and still showing up negative on PSMA PET scans.
One of the reasons that we talked about that at some length was that he suggested that Pluvicto / Lutetium-177 might be an option.
I asked about getting an Axumin scan or a Choline-11 scan, and he wasn’t in favor of doing either of those at the moment.
When to Start ADT
We also discussed when to start androgen deprivation (hormone) therapy (ADT). He didn’t have a set of specific criteria that he would use—e.g., specific PSA number, evidence of metastasis—but did focus in on the rate of PSA rise (PSA DT) and “patient motivations and preferences.”
What type of ADT
The doctor was a proponent of intermittent therapy in my case with six to twelve months on, then a similar period off. His goal would be to “maximize time off treatment” as long as my PSA is holding relatively steady and not going bonkers.
He seemed a tad hesitant to start with the combination therapy of ADT + ARPI (Eligard + Enzalutamide), but wasn’t opposed to it, either. He wasn’t a fan of trying the Enzalutamide alone because of its side effects (gynecomastia, in particular) and not seeing any substantial changes in long term outcomes.
Summary
I did share with the doctor the VA MO’s desire to start ADT + ARPI sooner rather than later, and he had a much lower sense of urgency in taking action. And, while I was a bonehead and didn’t explicitly ask him for his recommended course of action, the entire conversation led me to conclude that his preference was for continued close observation.
VA Oncologist
I technically didn’t meet with the oncologist; I met with a nurse practitioner who had reviewed my case with the oncologist just before (and during) my appointment.
Discussion
It was interesting that she opened the conversation with a quick review of my last appointment there, told me my PSA results from last week, and then said something along the lines of, “If you’re not ready to start ADT today, the doctor is okay with monitoring for another three months.”
At that point, I mentioned that I went to the UCSD MO the day before, and I spent a good chunk of time relaying how that meeting went.
I reminded her that I have the bone density scan in a few weeks and I intended to go through with that to establish a baseline even though we might not start ADT right away. She agreed.
I’m still meeting with the VA urologist on 23 June and want to get their thoughts on what’s next.
Summary
We’re going to do another PSA test in September, and the VA MO didn’t want to schedule an appointment with me until December with another PSA test just before that meeting, too. Interestingly, the VA MO also wanted to schedule a regular CT scan and bone scan ahead of the December appointment.
However, if the September PSA test jumps up significantly, we’ll revisit that plan based on the results. That may change doing the CT/Bone scans to another PSMA PET scan.
The Plan
In short, we’re going to kick the can down the road another three months.
More specifically:
Bone density scan – 17 June
Urologist appointment – 23 June
PSA test – First week of September
CT and Bone scan – First week of December
PSA test – First week of December
VA Oncology Appointment – 8 December
Summary
On the whole, I’m pleased with the plan as it stands right now. The UCSD MO emphasized the shared decision-making approach, adding in his notes, “Daniel is very well educated about his illness and understands there is no clearcut right and wrong answer.” Ain’t that the truth (about the no right or wrong answer).
Once I cleared the hurdles of getting set up in the UCSD system, I was impressed by the friendliness and professionalism of their staff in the department. They have a patient portal app that allows access to records and makes communicating about appointments—in both directions—quite easy.
One thing that I’ve noticed with both the VA and UCSD oncology departments is that their empathy and caring nature seems to be a notch or two above that of their respective urology departments. Not that the urology teams aren’t caring or empathetic; it’s just that the oncology folks seem to take it a step further.
I know the VA MO expressed a desire to take the lead on my case at my last appointment, and I’ll mention that to the urologist on the 23rd. And, for now, as pleasant as the experience at UCSD was, I plan on having the VA be my primary source of care.
We last left our hero with the beginning of a head cold after his scan and oncologist meeting. And, boy, what a head cold that turned out to be.
Normally, a typical head cold lasts a week or so and you’re back to normal. Not this time. This was the most stubborn virus, hanging on for three weeks and change. It was ugly. So ugly, in fact, that I went to the doctor for help.
The cold started out with a light fever and lots and lots of coughing. Of course, when you have your prostate plucked from your pelvis and they zap what’s left, stress incontinence is an issue. If I have a light cough, I’m generally okay, but with this virus, I was having deep coughs where it seemed as though I was trying to turn my lungs inside out. I had to switch to the heavy-duty incontinence pads and, even then, I blew out two of them with coughing fits, leaking into my underwear and jeans. Messy and not fun.
The doctor gave me something to calm the dry coughs, and that had a bit of a positive effect. But then my sinuses filled, my nose was running, and I was coughing up phlegm so I switched to something else to deal with that.
Long story shorter, it’s pretty much all behind me now, and that’s a good thing. Maybe I’ll go back to the COVID days and wear masks when riding packed transit or wandering the halls of hospitals.
While I was down for the count, I had plenty of time to dig into more about androgen deprivation therapy (ADT), its pros and cons, and the timing of starting it. Sadly, I could find information that supported pretty much any perspective you wanted, which really isn’t all that helpful.
On the whole, it appears the current thinking is to start ADT sooner rather than later, and to use a doublet therapy, i.e., ADT + ARPI. This seems to delay time to metastasis, but has the obvious cost of substantial side effects.
On a related note, I called UCSD on 30 April to set up a second opinion appointment with the medical oncologist that’s well-respected and that the VA called to consult on my case two years ago. Because I was already in their system, that helped a little. I had to update my insurance information, and they said they’d get back to me in 2-3 business days. They didn’t, so I called back today, 11 May. They put me on the “high priority” call-back list this afternoon to be called back “between now and 48 hours.” Okie-dokie. And they say scheduling appointments at the VA is difficult…
I’ve got a number of appointments coming up at the end of May and into June:
27 May – PSA Test and other pre-ADT labs ordered by the oncologist
2 June – Meeting with VA medical oncologist
17 June – Dexa Scan bone density scan for baseline
23 June – Meeting with VA urologist
With luck, I’ll be able to add the UCSD medical oncologist to that list as well.
I really want the PSA test results—specifically, the PSA doubling time—to be a guide into what happens next and when.
One of the other things that I dug into a bit when I was down with the cold was how many values to use when calculating PSADT. As expected, there were dozens of different answers. Grr. My pea-sized engineer’s brain decided that I’ll use the last four PSA values if they cover at least a year. To me, that would render more useful information that shows the latest trend versus loading in all data points that may skew the results to show something less aggressive. But what do I know?
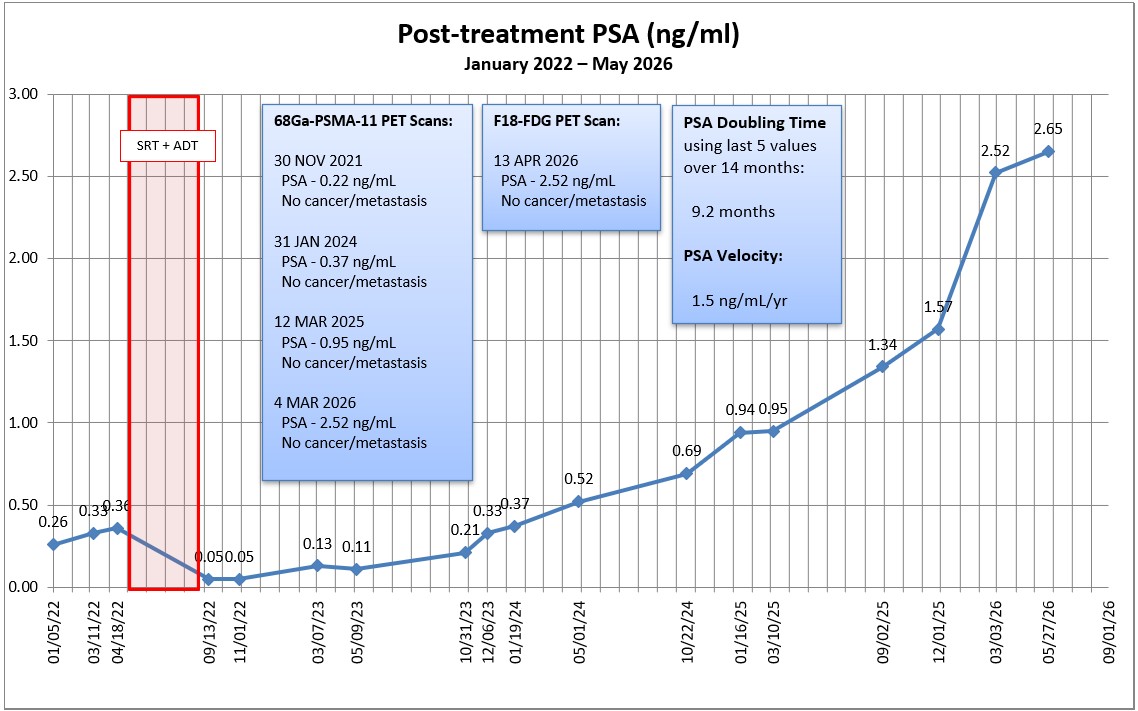
Using the Memorial Sloan-Kettering PSADT calculator and four data points over the last year, my PSADT is 8.9 months. Using a second calculator I found, it’s 8.21 months. For grins and giggles, I plugged in the last two years worth of data, and my PSADT was 10.4 months. Doing my research on ADT, PSADTs in the 6-9 month range seemed to be a trigger for action.
My PSA in March was 2.52 ng/mL, and I suspect it will be approaching 3.0 ng/mL at the end of May.
Obviously, this summer will be a series of data collection, evaluation, and big decision-making. Yippee! <sarcasm font>
One of the best things about keeping this blog going over the years is learning new information from you, the readers.
Recently, a reader left a link to this video in the comments of one of my recent posts. It highlights the work that two doctors from the National Cancer Institute (NCI) have been doing when it comes to assessing whether and/or when to treat patients with recurrent/advanced prostate cancer.
The video is about an hour long (I changed the playback speed to 1.25x to get through it a little faster) and was very timely for my current situation.
One of the interesting parts was the discussion on how to define metastatic prostate cancer. It’s still pretty squishy if you ask me.
It will be interesting to see what the oncologist says tomorrow.
Well, that was a surprise at 3 p.m. on Good Friday afternoon.
A resident from the urology department called to let me know that she had reviewed my email with the original urologist and, after consulting with the nuclear medicine department, they came to the conclusion that I made a strong case for me getting an alternate scan.
Unfortunately, the VA doesn’t offer the Axumin scans, but they do offer Fludeoxyglucose F18 (FDG) PET scans which are also reliant on PSMA for the ligand to attach itself to.
She said that the F18 ligand interacts differently than the 68-gallium does, so it’s possible that it will attach to the PSMA molecules on the cancer cells. (In a prostate cancer forum, one patient was in a similar situation. The 68-gallium scans didn’t work for him, but a Pylarify PSMA PET scan did.)
I know from earlier reading that F18 FDG scans aren’t as sensitive and may not work best in a recurrent cancer situation, but they definitely won’t pick anything up if we don’t do them. She offered to put the order in to do one, and I said yes.
I’ll give nuclear medicine a few days next week to receive and process the order before calling them to schedule the scan.
I thanked the doctor at the end of the call and she, in turn, thanked me for advocating for myself.
I’ll post more when the date is scheduled, and I’ll be putting my list of questions together for the medical oncologist appointment on 14 April.
The scheduler called this afternoon and we set up an appointment with the medical oncologist (MO) on Tuesday, 14 April 2026.
Hopefully, I can enlist the MO as an ally in trying to get an alternate scan to see if we can find out what’s happening with the cancer.
I did write to the urologist on Monday to let him know that I came away from the phone call with a different understanding of what’s next compared to what he wrote in his summary notes. (My emails are included in my medical chart, and I wanted to be on the record that we had a disconnect in communications.)
I did my best to keep my emotion out of what I wrote, and tried to present it as me wanting him to further explain his viewpoint. I wrote, in part:
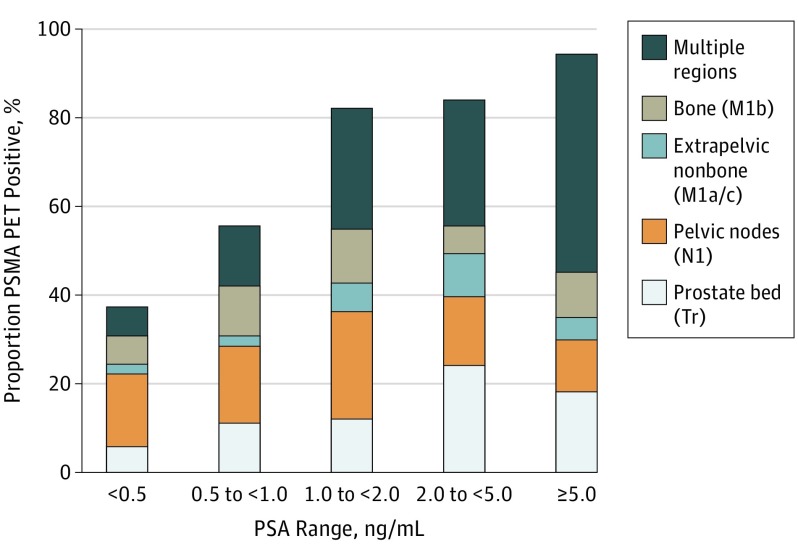
I agree with you that PSMA PET scans have become the gold standard for most patients. But we also know from multiple studies that 5% – 10% of patients don’t express PSMA and the scans won’t work for them.
I believe the fact that I’ve had four 68-Ga-PSMA-11 PET scans that haven’t located my cancer is strong, objective evidence that I may be in that small group of patients for whom the scans don’t work (barring any other possible test/proof that shows I don’t express PSMA). The last two scans should have had an 80% – 90% chance of detection at my respective PSA levels.
Please help me understand more definitively why you believe PSMA PET scans work for me, and what further evidence you would need to convince you that I may be in that group for whom the scans don’t work.
Finally, you stated that there was “limited likelihood that Axumin would provide additional clinically actionable information.” How would we know that unless we try? Axumin scans have an 80% chance of detecting something at PSA levels over 2.0 ng/mL.
We banked on PSMA PET scans to provide that clinically actionable information, yet time after time, they haven’t.
I’ll let you be the judge as to whether I kept the emotion out of my email. Again, the email to him went out Monday afternoon, so I wouldn’t expect a response for a few more days (if he’s even inclined to respond). I’m not sure if it was coincidence or if he pushed Oncology to call me because I did note at the end of my email that I hadn’t heard from them yet.
We’ll have to see how this plays out. More to come.
As I was driving to the barber to get my hair cut (both of them), my phone rang. Normally, I avoid phone conversations when I’m driving—even the hands-free, Bluetooth variety—but when the Caller ID popped up on the infotainment screen as being the VA Medical Center, I answered because I thought it might be the Oncology scheduler calling to set up an appointment.
Instead, the call was from the urologist I met on Tuesday to talk about his research and efforts to pursue an Axumin scan. (I sent an email to him yesterday saying that I did a little legwork for him and learned that UCSD still does Axumin PET scans in case the VA didn’t.)
In a nutshell, he contacted the VA nuclear medicine department and, according to him, they were very elusive with him in saying whether they even had the ability to do the scan at the VA and, even if they did, if they would do it considering the PSMA PET scans have replaced it in their minds.
Then the doctor again put his faith in the PSMA PET scan and thought that the Axumin scan wouldn’t provide any useful information. He also mentioned that he looked at the 10% of patients not having PSMA protein and said, from his quick research, it seemed to only been identified in a single study. Unfortunately, that was said at a time when I was more focused on driving than listening, and I’m sure I didn’t fully understand what he was trying to convey.
I was finally able to safely park and give 100% of my attention to the conversation, and he said one other thing that puzzled me. He seemed confident that, because my PSA was rising, I did, in fact, have the PSMA protein. I’m not sure that I agree with that and need to do some digging.
We did talk about having a Pylarify PSMA PET scan which uses a different tracer than the 68-Ga-PSMA-11 PET scans. He thought that that could be a possibility, but wasn’t sure that the VA offered it yet. He knew it had been FDA-approved, but thought that the VA hadn’t developed the protocols for its use yet. I mentioned that when I spoke with UCSD yesterday, they said they had the ability to do Pylarify scans, too.
I asked him about how I might get a referral from him/the VA for me to get the scan on my own, and he thought that there may be a number of bureaucratic hoops to jump through to make that happen, including determining if something was “medically necessary.” He wasn’t exactly sure of the process, especially if I was going to use my own insurance (Medicare).
I just wanted him to confirm that, in his view, there was value in getting a scan to learn the location of the cancer and what it’s doing. He agreed.
I told him that my goal was to find the cancer and, if there were one or two lesions, to do spot radiation to knock them down if they’re in a suitable zapping location. That may help delay the start of ADT. (Or not. I’m not sure if they put patients on ADT when going after oligometastatic lesions.)
Finally, he did ask if I had been scheduled with the oncologist yet, and I have not. He was interested in hearing what they had to say about scans.
Needless to say, the waters have been muddied and I’m a little less confident that I know what’s going to happen next.
I’ll send him an email in the morning recapping our conversation, with an emphasis on his agreement that having a scan at this point is important. Translation: Medical necessity. I’ll also let him know that I’m open to trying any scan that he thinks will work.
I may also ask him to explain again why he is convinced that I have the PSMA protein and why he’s skeptical of the 10% number.
I’ll also try to connect with the oncology schedulers and get that appointment on the books.
I may also look at what it takes to get myself in as a patient at UCSD through either their urology or medical oncology departments. Because UCSD did my salvage radiation therapy in 2022, I may still be in their system, so it may be less difficult than starting from scratch. I’ll have to figure out how to share my VA health records with UCSD if needed.
Those of us of a certain age may remember the “Stump the Band” segment on the Johnny Carson show, where audience members asked the band to play some obscure song. Well, today was my turn at “Stump the Urologist.”
It was a very productive meeting that lasted nearly 40 minutes which was unusual. I came equipped with hard copies of my PSA chart, the MSKCC PSA doubling time (PSA-DT) calculator results, and my list of questions. He was impressed and really pleased with the chart in particular.
We started talking about how my four PSMA PET scans were all inconclusive, and I steered the conversation to whether I might be one of the 10% for whom PSMA PET scans don’t work. He seemed to be a bit skeptical at first, but he also said it was a possibility.
Given that my PSA increased substantially and my PSA-DT was decreasing, I wondered if it would be better to jump into ADT sooner or if there’s still value in trying to find the cancer’s location with imaging. He was of the opinion to continue to try to find it before starting ADT.
I had a series of questions that really dealt specifically with ADT, and he said it was a bit premature to think about those and that they would be better answered by a medical oncologist. I knew that I was jumping the gun with some of them, but I thought I’d ask anyway. During that part of the conversation, I did mention that I tolerated the ADT probably better than most when I had it for my salvage radiation therapy, but that I wasn’t eager to jump into it earlier than necessary.
After that, he took control of the conversation and asked me about my status when it came to sexual function and incontinence, and offered up options to deal with both if I was interested.
Then we returned to the topic of next steps, and that’s where I played “Stump the Urologist.” (Who, by the way, was a full-blown internist and not a resident.) He grabbed my PSA chart and excused himself for a few minutes as he went off to consult with the department head.
When he returned, I was a bit surprised when he put his faith in the results of the PSMA PET scan, saying it has the best sensitivity and the best specificity of any scan out there. He said that they had moved away from the Axumin scans because they were the old technology.
I politely pushed back, reminding him that a PSMA PET scan should have had an 80% – 90% chance of finding my cancer at my PSA level if I had the PSMA protein for the 68-Gallium tracer to lock onto. But if I don’t have that PSMA protein, the sensitivity and specificity of the scan won’t matter because nothing will ever light up. He really couldn’t argue against that.
I went back to the topic of ADT and mentioned that I met with a medical oncologist (MO) two years ago, and received conflicting opinions on when to start ADT. The MO said she would start my ADT when my PSA hit 2.0 ng/mL (a urologist said she wouldn’t start it until there was evidence of metastasis). Today’s urologist said he looks for one of three “triggers” to begin ADT: PSA > 10.0 ng/mL 😲; PSA-DT less than six months; or evidence of metastasis.
I also mentioned that the VA MO that I saw two years ago was a general oncologist and not someone who specialized in genitourinary cancers and, as helpful as she was, she had to consult with a UCSD MO who specifically deals with prostate cancer. I sowed the seed of eliminating the VA MO as a middleman if they have to consistently consult the UCSD doctor (who is highly regarded in the field), and suggested that I could just see him directly. I’m not sure if that will take root.
Finally, I did ask a very basic question given how elusive this has been: Is this even cancer? He said that, if I hadn’t had a prostatectomy, that there might be other explanations for the rising PSA. But he was confident that we are, in fact, dealing with cancer.
That led to a follow-up question of: Is it metastatic? Based on the information we have, he said it’s not. He seemed to squirm a bit when I asked about it being micro-metastatic, because, in his mind, that wasn’t very well-defined.
Before mapping out a plan, I have to admit that my ego puffed up a tad when he said, “You’re the best educated patient I’ve seen in weeks.” He also admitted that my case was a bit puzzling to them and not something they routinely see.
We agreed on three actions:
The doctor is going to explore how and where I can get an Axumin scan, and if the VA will authorize it if I have to go outside the VA. That may take a day or two to get an answer. I mentioned that I’d be willing to use Medicare and go out on my own if necessary.
He is doing a referral to get me seen by the VA oncology team to get them familiar with my case. I suspect it will take a few days to hear from the scheduler.
We do another PSA test in June and meet to see where we’re at.
All in all, this was a good meeting with a robust discussion about my case that has all of us scratching our heads as to what’s going on and what to do next. Frustrating? Yes, to a degree. But, as we discussed during the meeting, nothing is black-and-white in the world of prostate cancer.
More to come.
Be well!
For my readers outside the U.S. who may not be familiar with Johnny Carson, I was going to link a random video clip of his “Stump the Band” segment above and, when I searched YouTube, this—of all clips—was the one that popped up first. I think you’ll see the related humor in it once you watch it. 😂
Header image:Anza-Borrego Desert State Park, California
The next time I come down with the flu, I’ll be sure to send out some insider trading information: Buy stock in incontinence pads, ASAP.
Just over three weeks ago, the flu bug came home to roost, and it kicked my ass. Chills, aches, fever, and coughing. Lots and lots of coughing. The worst symptoms lasted about eight days, but the coughing remained after the chills, aches, and fever were gone.
Of course, coughing is one of my stress incontinence triggers. A small, light cough, and I can hold my own. But these were heavy, cough-up-your-toenails coughs which caused significant incontinence issues. It sucked. I was going through multiple incontinence pads each day and night.
A friend had the same bug back in December, and she said it took three weeks for the coughing to subside. That seems to be my experience, too. I’m finally just about back to normal.
Oh well. I survived and it’s behind me.
In three weeks, I’ll go for my next PSA test (2 March) and the PSMA PET scan (4 March). It will be interesting to get the results of both.
I’m hoping that the PSMA PET scan shows something this time. My last PSA on 1 December 2025 was 1.57 ng/mL, and I’m guessing this one will be approaching the 1.7 to 1.9 range. At that PSA level, there should be a slightly better than 80% chance of finding something.
An old boss was known for saying, “If you can’t stand the answer, don’t ask the question.” As eager as I am to have an answer, I’m not so sure how I’ll respond if the answer comes back, “It’s metastasized.” Logically, I know that’s the likely next step in the progression. Psychologically—emotionally—I’m trying to prepare myself for that possibility.
Yes, I know that hormone therapy and other advanced treatment options will be able to keep me around for a long time even if it has metastasized, so I’m not worried about keeling over in the next six months. I guess it’s the fact that I’ll have passed a point of no return, and my future will become a balancing act between slowing the cancer’s spread and maintaining a decent quality of life. C’ést la vie.
Of course, if the PSMA PET scan comes back without any evidence of cancer or metastasis, it may be time to try a different imaging method. That will kick this can a few more months down the road.
With luck, it will all come together when I meet with the urologist on 24 March and we go from there.
Be well!
Header image:Silver Strand State Beach, Coronado, California
I held off on this post until I was able to get my PSMA PET scan scheduled this week.
I had been playing phone tag with the scheduler and, when I finally got to speak with him, I learned that they normally don’t schedule until 30 days in advance of the request date. Because the order for the scan said March, they weren’t going to call until next month. Fortunately, because we were already on the phone, the scheduler went ahead and put me on the calendar for 4 March 2026.
That should give enough time to interpret the results before my 24 March appointment with the urologist. I’ll go for a PSA test just before the scan on 2 March.
I continue with my pelvic floor physical therapy every other week. I’m not sure that it’s been having an effect on my incontinence, so I’ll have to ask how long it takes before I have any truly noticeable improvement.
Other than that, there’s not much else to report. Just another day living with prostate cancer.