It’s been a busy two days hanging out at the doctor’s offices between the scan and the oncologist. Here’s a summary of each, my final thoughts, and a quick explainer about hormone therapy for the uninitiated at the end.
18F-FDG PET Scan
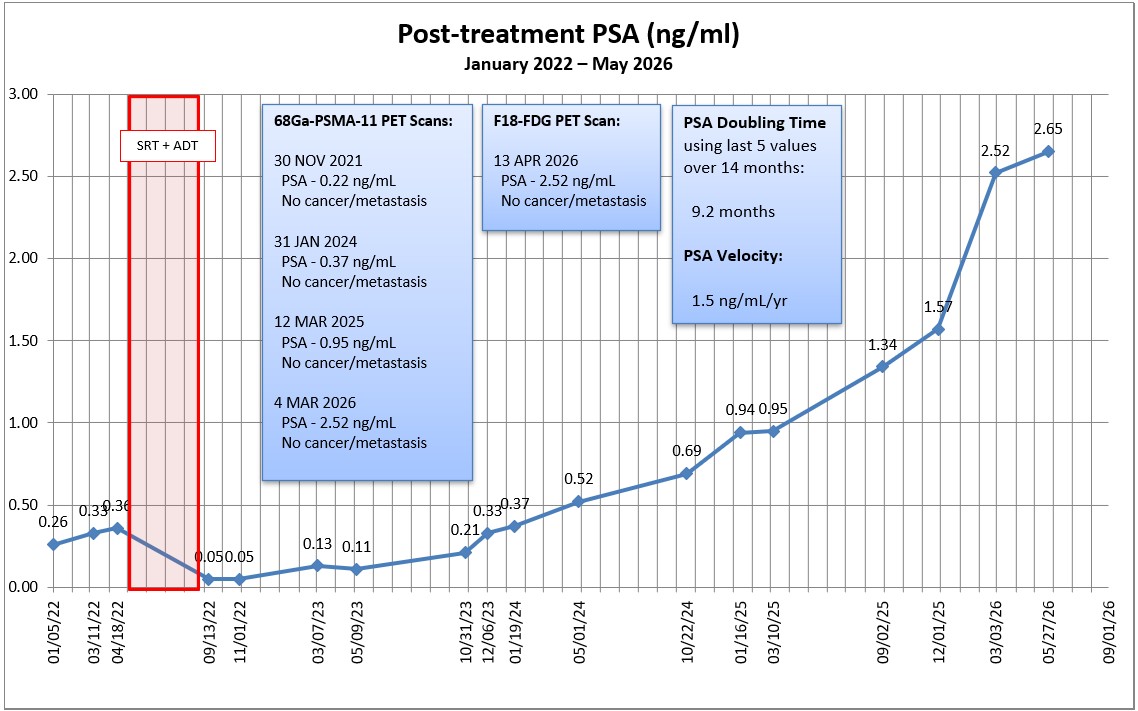
“No evidence of metabolically active malignancy or metastatic disease.”
Well, I hate to say it, but I’m not necessarily surprised by that result. I didn’t have high hopes of getting a definitive answer going into the scan given its lower sensitivity and lower specificity, but I thought it was definitely worth the effort.
As far as the procedure itself was concerned, it was slightly different than the 68Ga-PSMA-11 PET scan. I had to fast for at least 6 hours (no food, just water) before the injection of the 18F-FDG tracer. They also had to measure my blood glucose level to ensure it was under 200 mg/dL (it was). If it was over, the scan would have been canceled.
There was a one-hour waiting period for the tracer to distribute through my body, and the scan itself took 45 minutes. Seeing as I had to get up at 4:30 a.m. for my 7 a.m. appointment, that hour in the recliner was much needed.
Oncologist
I actually met with two medical oncologists this morning, the resident about to complete his training (MO Jr.) and the full-blown MO Sr. who focuses on prostate and breast cancer. It was a good, nearly hour-long discussion. In a nutshell:
- It was disappointing that the imaging didn’t show anything and, even though it would be nice to know where the cancer is located, MO Sr. felt it was time to start systemic treatment.
- MO Sr.’s triggers for starting hormone therapy were a PSA greater than 2.0 ng/mL (I’m at 2.52) and a PSA doubling time less than 9 months (I’m at 8.9 months).
- MO Sr. said that, with my numbers, I’m at “higher risk” for this to get away from us and metastasize.
- MO Jr. said that the window for curative options has closed and that treatment going forward would be “palliative.” (I already knew that curative options were out the window.)
- Both agreed it’s time for them (Oncology) to take the lead on my case at this point, with Urology still available in a supporting role.
- Both suggested dual therapy involving androgen deprivation therapy (ADT) using Eligard (leuprolide acetate) and and androgen receptor pathway inhibitor (ARPI) using Xtandi (enzalutamide) as the current standard of care. [See explanation below if you’re unfamiliar.]
- MO Sr. also suggested intermittent therapy over continuous therapy, using a 9-month schedule to start.
If she had her way, I believe MO Sr. would have had me start the therapy in the next week or so. I tapped on the brakes on that idea. I told her that Urology wanted another PSA test done in early June, and I thought it would be good to get that done before starting anything. Also, I’m traveling in May and I simply wanted to postpone anything until after I return. Six weeks won’t make that much of a difference.
We agreed, in concept, to the following:
- No more scans to try to located the cancer for now.
- Get pre-therapy lab work done the week after Memorial Day to establish baseline testosterone and PSA levels (among others) ahead of therapy.
- Get a Dexa bone density scan to get a baseline prior to starting treatment (extended ADT can weaken bone density).
- Meet on 2 June to review the results and make the final decision as to whether to start treatment.
Final Thoughts
It’s only been a few hours since the meeting, and I’m still trying to absorb it all and process it. Of course, after 15+ years of dealing with this, I knew we would eventually get to this point. Am I ready or willing to take the advice of the National Cancer Institute doctors in the video I shared recently to just monitor and delay treatment? I don’t know. It’s something that I’ll have to contemplate over the next six weeks or so.
I will say that I was pretty impressed with the Oncology Department as a whole. You’re assigned a care coordinator and given their direct phone number for all questions or concerns, and both doctors were good at listening and engaging in a real conversation. It seemed like they were a bit more empathetic over all, and that’s a good thing.
Certainly a lot to take in in the days and weeks ahead. I’m open to thoughts and feedback.
Be well!
—Dan
Hormone Therapy Explained
For those who aren’t really familiar with how prostate cancer works and what role hormone therapy plays, here’s a grossly over-simplified explainer.
Prostate cancer feeds off of testosterone and, as long as there’s a supply of testosterone, the cancer will continue to grow.
There are two ways to deprive the cancer of testosterone. The first is to stop or slow the production of testosterone. The second is to block the cancer cells from receiving the testosterone. The current standard of care is to use both methods simultaneously.
Let’s say the cancer cells are in the bottom of your favorite travel mug, thirsty for testosterone. If you put the mug under running water from your tap, the cells get the water (testosterone) they need and the cancer grows. But if you turn the tap off, the water (testosterone) stops flowing, and the cells in the bottom of the mug can’t grow. This is called androgen deprivation therapy (ADT).
The other way to stop the cancer cells in the bottom of the mug from getting water (testosterone), is to simply put the lid on and block the water from entering the mug. This is called androgen receptor pathway inhibitors (ARPI).
If you do both simultaneously, you can really slow the growth of the cancer. But we also know that some taps have slow leaks that drip water and, if the lid is slightly open, water (testosterone) and still make it to the cancer cells inside the mug.
There are two ways of turning the tap off. One, an orchiectomy, is a radical, surgical and permanent removal of the testes. But the adrenal glands also produce a small amount of testosterone, too, so the flow isn’t completely stopped.
The other is to use an ADT drug to have the brain tell the testes to stop producing testosterone. The drug is given via an injection in typically one, three, or six month doses, and it has significant side effects: hot flashes, mood swings, fatigue, loss of libido, loss of muscle strength, and loss of bone density, to name a few.
The way to put a lid on the mug is through an ARPI drug that’s usually taken in pill form daily. In my case, MO Sr. was recommending Xtandi (enzalutamide) as the ARPI. It has its own host of side effects: muscle and joint pain, fatigue, falls and bone fractures, headaches, high blood pressure and others.
The good news is that this combined treatment option can keep the cancer at bay for years (as long as you stay on it for years). However, at some point, the cancer can become resistant to the drugs, and you may have to move to stronger treatment options like chemotherapy.
Again, this is an oversimplification for those new to the topic.
Header image: Anza-Borrego Desert, California