I held off on this post until I was able to get my PSMA PET scan scheduled this week.
I had been playing phone tag with the scheduler and, when I finally got to speak with him, I learned that they normally don’t schedule until 30 days in advance of the request date. Because the order for the scan said March, they weren’t going to call until next month. Fortunately, because we were already on the phone, the scheduler went ahead and put me on the calendar for 4 March 2026.
That should give enough time to interpret the results before my 24 March appointment with the urologist. I’ll go for a PSA test just before the scan on 2 March.
I continue with my pelvic floor physical therapy every other week. I’m not sure that it’s been having an effect on my incontinence, so I’ll have to ask how long it takes before I have any truly noticeable improvement.
Other than that, there’s not much else to report. Just another day living with prostate cancer.
Late last week, I received a text message asking if I would like to move my urologist appointment from 30 December to today, 23 December, and I agreed.
My appointment was at 3:15 p.m., and I arrived around 2:45 p.m. As I’m walking up to the check-in kiosk, my cell phone rings, and it was the urology department wanting to confirm that I’d be there. That’s the first time that that’s happened, and I told the nurse that I was checking in as we spoke. “Great! We’ll come out and get you.” Apparently, they were antsy to get out of there early on the day before Christmas Eve. So was I.
The head of the department was the one who saw me this time, and we had a really good conversation. Some of the key takeaways:
She was concerned about the increase in my PSA but not panicked, even initially suggesting we just continue to monitor it.
We talked at length about doing another round of imaging to see if we can determine the location of the cancer.
We agreed to do another PSMA PET scan, and we negotiated doing one in March 2026. (She thought that Nuclear Medicine might push back on doing one sooner, i.e., within a year, as the last one I had was in March 2025.) She also mentioned the possibilities of other imaging should the PSMA PET scan come up with no evidence of cancer/metastasis for the fourth time.
We talked about the timing of starting androgen deprivation (hormone) therapy. She wouldn’t start it until there was evidence of metastasis, but was open to starting it earlier if I really wanted to do so.
Lastly, we reviewed my stress incontinence and nocturia issues and talked about my pelvic floor physical therapy.
It was one of the more thorough discussions that I’ve had at the VA, and I’m okay with the plan coming out of the meeting. I’ll go for another PSA test on 1 March; hopefully get the PSMA PET scan scheduled in early March; and have a follow-up with the urologist on 24 March.
I’m glad I got this out of the way before the holiday. I’ve got my answers, plus it frees up next week for me to go out an play if I want.
Merry Christmas, Happy New Year, and be well!
Header image:Hotel del Coronado at Christmas, Coronado, California
In a nutshell, we’re punting the ball another three months down the road.
The doctor commented on the continuing rise in my PSA and said after consulting with the doctor who saw me last time, said that he wanted to recheck my PSA in six months and “wait a year” for another PSMA PET scan. I should have asked for clarification on that, but I think he was referring to waiting a year after my last PSMA PET scan in March 2025 and not a year from today.
I wasn’t entirely comfortable with waiting another six months, so we agreed to test PSA again in December (three months after my September test) and go from there.
We also talked about spot radiation if anything pops up on the scan. He seemed a bit reluctant for that to be an option, and went straight to starting hormone therapy. It’s as though he was making the transition from curative options to management options, and, to be perfectly honest, I believe I made that transition in my own mind once the salvage radiation failed. That doesn’t mean that I wouldn’t try zapping a lesion or two if they popped up on the scan depending on location (no more zapping to the pelvis and risking further bowel complications).
We did talk about my experience with hormone therapy during the salvage radiation, and the timing of starting it this time around. In that discussion, he brought up the topic of bringing in a medical oncologist at some point depending on the scan results and my PSA test results.
We talked at length about my urinary frequency and some options for that. He suggested some pelvic floor therapy might be beneficial, so I said I’d be willing to give that a try.
Overall, I’m okay with where we’re at and the planned course of action for now. I’ll go for my PSA test in early December, and if there’s another significant jump, I’ll press for the PSMA PET scan to be done sooner rather than later.
My next scheduled urologist appointment is 30 December 2025.
I had my post-PSMA PET scan visit with the urologist today, and I wasn’t really sure what to expect going into it.
The doctor (same as last time) shared the scan results saying that they’re something I should celebrate. I mentioned, though, that I have had three scans and were inconclusive despite the rising PSA numbers. He was quick to reply by saying that the scan not showing evidence of prostate cancer or metastasis was conclusive.
I understand where he’s coming from, but until we know where the cancer is, I’m going to have a difficult time accepting that perspective.
I did ask whether there was some sort of test that can determine if my cancer doesn’t express PSMA, and he said that there wasn’t. Something in my pea-sized brain tells me I need to double check him on that.
I also asked if there could be another explanation beyond the cancer that would explain my rising PSA. He ruled out the possibility of some residual prostate tissue being left behind after the surgery as being the cause based on my PSA kinetics over time.
In terms of what’s next, we’re kicking the can six months down the road for another PSA test and follow-up. I was a bit surprised that he wanted to wait six months, and suggested doing the test in three or four months. He was a bit insistent on the six month window. He felt comfortable with my current situation—the slight increase in my last PSA test from the previous one and my PSA doubling time—that waiting six months wouldn’t be a problem. He also argued that having a longer period between tests would better reflect what’s going on.
As we wrapped up, he reminded me that the scan results were good news, and I know that he’s right in that regard. I’ll work on changing my own perspective going forward (even though those little cancer bugs are still doing their thing inside me.)
My follow-up appointment is on 30 September 2025.
That’s it for today. Be well!
Header image: Cherry Blossoms, Japanese Friendship Garden, San Diego, California
On the whole, the news is good. My PSA just barely bumped up from 0.94 ng/mL in January to 0.95 ng/mL in March and, taking the last five readings, that increased my PSA doubling time from 7.7 months to 10 months.
The PSMA PET scan revealed “no evidence of prostate cancer or metastatic disease.”
So, if the news is good, why am I “so over this?”
I was really hoping that this third PSMA PET scan would bring some clarity as to where the cancer was located so we could know how to proceed—even if it meant revealing metastatic disease. It’s frustrating because we know the cancer is somewhere and because we know the PSA almost tripled between 19 January 2024 and 16 January 2025, but we don’t have enough information to do anything about it. It’s just more waiting in limbo.
Of course, having had three PSMA PET scans all turn up negative makes me question if I’m in that “lucky” category of ten percent of patients whose prostate cancer doesn’t express PSMA, making the scans useless for me. It’s something that I’ll definitely discuss with the doctor at my next appointment on 1 April 2025. I vaguely recall that there’s some sort of genomic test that may be able to assess if I really do fall into that ten percent. I’ll have to do some research on that.
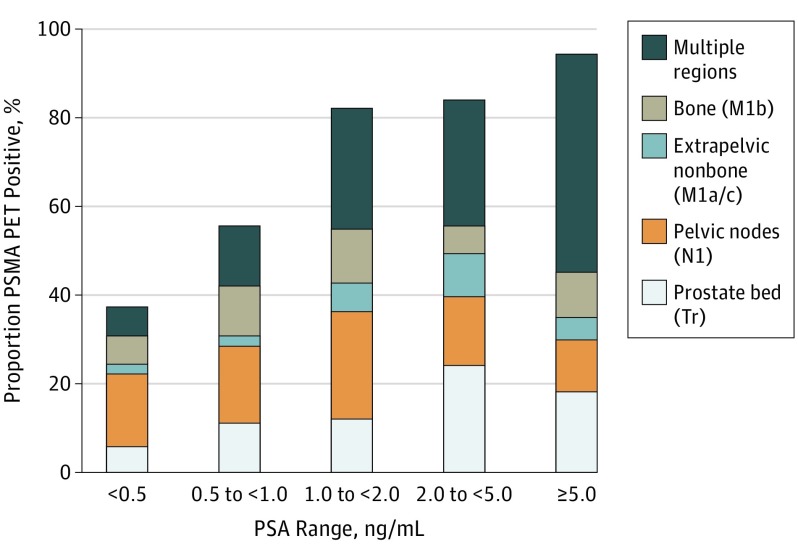
Maybe, too, I’ve placed too much faith in the scan’s ability to detect anything at my PSA level. But with a PSA level hovering around 1.0 ng/mL I thought we would have a decent chance of detecting something (chart below).
Detection Rate on a Patient Basis Stratified by PSA and Region Tr indicates prostate bed only; N1, pelvic nodes only; M1, extrapelvic only. Proportion of patients with 68Ga-PSMA-11 PET positive findings were stratified by PSA range and region of disease in accordance with PROMISE. https://pubmed.ncbi.nlm.nih.gov/30920593/
Needless to say, I’m truly glad that my PSA didn’t rocket even higher and that my scan didn’t light up like Times Square. Having definitive answers, though, would be the icing on the cake.
As far as the PSMA PET scan itself, it was pretty easy and took two hours to go through the entire process. I was instructed to drink 500 ml of water starting 2 hours before the scheduled scan time, and that was the only preparation needed.
I arrived at the hospital at 8 a.m. and was brought back to a radiation-proofed exam room where the technician started and IV at around 8:15 a.m. The 68Ga tracer was ready for injection around 8:40 a.m.
Around 9:30 a.m., the technician brought me back to the scanner where I got positioned on the bed and we began the scan which took 45 minutes. The scanner was very quiet (I could have dozed off) and large enough that it wasn’t claustrophobic. I was out of there by 10:15 a.m. and on my way home. Piece of cake.
On a related note, this was the longest it’s ever taken me to get the PSA test results posted online (hence the delay in this post). I actually called the clinic to get them over the phone because they still weren’t available online today (Thursday). The nurse I spoke with was very helpful and said, “We’re facing staffing issues and, well…” stopping herself in mid-sentence, probably remembering that the call was being recorded and not wanting to make a statement about the current environment for VA employees at the moment. I fear that this may be a precursor of things to come.
You may have overachieved when your doctor asks, “Are you a urologist?”
I had a good meeting with the real urologist this morning, and it appears that he actually read the questions I sent to him in advance. That made the discussion easier.
First on my question list was whether a PSMA PET scan was warranted. He agreed that it was, and we’re going to try to get that scheduled soon. He thought that, with my PSA at 0.94 ng/mL, there would be a better chance of actually finding something this time. The only concern is that the VA has required a bone scan ahead of the PSMA PET scan in the past, and he’s going to see if we can skip that. It may take several days for the schedulers to call me.
We did discuss the possibility of further radiation if a lesion is found away from the pelvis. I mentioned that I had had blood in my stools and mild radiation proctitis discovered (and addressed) during my recent colonoscopy. He was not keen on further radiation to the pelvis under those circumstances. Neither am I.
My next question was about the timing of beginning androgen deprivation therapy (ADT). He was pretty squishy on the timing, not knowing exactly where we’re at. I mentioned that, a year ago, the urologist told me that we’d start when my PSA hit 2.0 ng/mL, but the medical oncologist suggested holding off until metastasis. He generally agreed with the concept of starting it later so that the cancer doesn’t become resistant to it prematurely, with one caveat.
He seemed to give more weight to my PSA doubling time than did other doctors, and that’s when he asked me if I was a urologist. I had presented him my graph showing my PSA progression, and it showed my PSA doubling time. “How did you know how to calculate it?” I told him that I used the Memorial Sloan-Kettering PSA doubling time calculator. To him, my PSADT of 9 months was creeping into “concerning” territory, and might make him a little more inclined to start ADT earlier.
I asked him, “At what point do we call this metastatic disease?” and, “When should we get a medical oncologist (MO) involved?” To the first, he said that all we know is prostate cancer is somewhere in my body, but wouldn’t go so far as to call it metastatic yet. To the second, he was open to brining in a MO if the results of the PSMA PET scan warranted it.
We agreed to the following plan:
Get a PSMA PET scan and meet again in six weeks to review the results.
Get an updated PSA test before the six week review.
Let the results of the scan determine if we get the MO involved at that point.
I have the six-week follow-up appointment scheduled for 1 April 2025. My concern is getting the PSMA PET scan scheduled and completed before then. If I need a bone scan in advance of it, that may complicate or delay the PSMA PET scheduling further. If push comes to shove, I already had an appointment scheduled with urology on 8 May 2025, so that’s not that much of a delay if we can’t get everything scheduled before 1 April. 2025.
It was a productive meeting from my perspective, without any surprises.
More to come as we get things scheduled.
Header image: Cuyamaca Rancho State Park, California
I’ve been debating whether to write this post but figured that I’ve never shied away from sharing the gory details of the total prostate cancer experience. So if you don’t want to read about my latest adventure with incontinence, you can check out the trip report of my trip to Death Valley last week.
In fact, the issue began as a result of my trip to Death Valley.
After four days of standing in the middle of the desert pretty much solo the entire time, I returned home Wednesday evening. Thursday morning, I can off to the clinic for my PSA test (it took 7 minutes and 38 seconds from check-in to walking out the door). But by Thursday afternoon, I was feeling a bit wonky.
By Thursday night, I was down for the count with a full-blown head cold/flu. I was both baffled by how I contracted it, and annoyed that I had. It had been several years since I’ve had a cold or flu.
Unfortunately, one of the symptoms that hit me hard and caused the incontinence issues was a nagging tickle in the back of my throat that had me coughing pretty consistently and, in many cases, pretty intensely. It sucked.
It sucked because coughing is perhaps the greatest trigger for my stress incontinence. The harder I cough, the more I leak.
I wear Depend Shields in my daily life, and I can get by with one or two pads a day. But by the weekend, the coughing and resultant leaking exceeded their capacity. I had one coughing fit that had me fill the pad, overflow, and soak my jeans. Not fun. Through the weekend and into early this week, I was going through multiple pads a day and doing several loads of laundry.
I toyed with the idea of running to the store to get Depend Guards, the pads with more absorbency and capacity, but I didn’t want to risk embarrassing myself in the middle of Aisle 12 at the grocery store. Plus, I was probably as contagious as Typhoid Mary, so that wouldn’t have been a good thing, either.
I was taking some cold/flu medicine that helped reduce the cough—the root cause of my issue—and I just rode out the storm for a few more days. Today, a week after this all kicked in, I’m back to my good ol’ self getting by with the occasional drip and dribble.
The lessons learned for me are to keep the cough medicine on hand to help reduce the root cause, and to keep a supply of Depend Guards on hand to do a better job of controlling the mess.
Now you know why I may have been hesitant to share this. But, hey, it’s for educational purposes, right?
On a related note, I was successful in getting my appointment to review my PSA results moved to an earlier date. It’s now 18 February 2025 (four weeks is better than four months). I’m okay with that.
Unless you’ve been living under a rock the last two weeks, you already know that southern California has been ablaze with wildfires. Luckily, up until this point, they have stayed clear of San Diego for the most part. Until today.
This little gem popped up about 6 miles / 10 km from my house this afternoon:
View of the Border Fire on Otay Mountain taken from the vacant lot down the street from my house.
It’s grown to about 600 acres / 240 hectares in about six hours, and we’re expecting high Santa Ana winds this evening. It’s in a very mountainous area, and air crews have been working the scene all afternoon. Luckily, it’s adjacent to a large reservoir, so there’s plenty of water for the helicopters to access. We also have rain in the forecast for the weekend for the first time in months (San Diego has had the driest start to the wet season since they began keeping records in 1850. We’ve had only 0.14 inch / 3 mm of rain since 1 July 2024.)
Of course, I’m concerned and I’ve made preparations to leave if need be. But given the location, the fact that the reservoir is between me and the fire, and the prevailing winds are keeping the smoke south of me, I’m hopeful that my neighborhood will be unaffected.
I’ll keep everyone updated over the next day or two.
Be well.
Header image: Courtyard at The Ranch at Death Valley National Park, California
I jumped the gun a couple of days and went for my PSA lab work Thursday morning on 16 January. (The three month date since the last PSA test would have been 22 January.)
As a refresher, my PSA in October was 0.69 ng/mL; it’s now 0.94 ng/mL.
I’m going to have to get a little aggressive with the medical team in terms of appointment scheduling. In October, we agreed to retest in three months and go over the results, but the schedulers didn’t have any open appointments until May 2025. Needless to say, that’s too far out so I’ll have to cajole my way into a canceled appointment or ask for a virtual / telehealth appointment sooner.
With my PSA as high as it is, I suspect that another PSMA PET scan would finally reveal some useful information that we can use to plan treatment options.
Header image: Devil’s Golf Course, Death Valley National Park, California
I’ve used the prostate cancer forums on the website HealthUnlocked to help gain other patient experiences as I move deeper into the world of advanced prostate cancer.
Recently, one of the forum moderators posted a link to this article:
It’s a rather blunt—perhaps even controversial—look at how patients research their diseases and treatments, but it does make you think about your own approach to becoming an educated patient and perhaps some of the pitfalls in doing so.
You may find it interesting. Or not.
Header Image: San Diego skyline from Coronado, California
No one can say I do things half-assed. I got a perfect 9/9 score on the Boston Bowel Preparation Scale. Clean as a whistle! 🙂 (I didn’t even know that there was such a scale.)
Yesterday’s colonoscopy went well, although it was a little different from the last one I had six years ago. The last one, I was knocked out with anesthesia and don’t remember the procedure at all. This one, I had “moderate (conscious) sedation” and was able to have conversations with the team and watch the procedure on a monitor, although my mind was drifting in and out of focus throughout.
Before we started, I had a good conversation with the doctor about my salvage radiation therapy and the possibility of radiation proctitis given the occasional blood in my stools. She was appreciative of the detailed information to help her in doing the procedure. I really stressed that I didn’t want the scope or the inflation of my colon to do more damage than what may already be there.
There were two polyps that were removed during the procedure and will be sent off for pathology. The first was in the transverse colon, and the second in the sigmoid colon, not far from the rectum. (I didn’t think to ask how long it will take for the pathology to come back, but I’m assuming it will be about two weeks.)
The sigmoid polyp was described as, “erythematous and friable.” Erythematous means the mucosa is red and inflamed due to a buildup of blood in dilated capillaries; friable describes how easily the mucosa can be damaged by a biopsy instrument or endoscope.
Because I didn’t read her printed report—with 13 color photos and map of my colon—until I got home, I didn’t get to ask if she thought that could have been caused or aggravated by the radiation therapy being closer to the rectum.
She also found “a few non-bleeding small angioectasias in the rectum, consistent with chronic radiation proctitis,” which are dilated, thin-walled blood vessels (think spider veins) that can occur anywhere in the gastrointestinal (GI) tract. I watched her zap those with “argon plasma coagulation (APC).” She described that as cauterizing the vessels to stop them from possibly bleeding into the GI tract.
Pending the outcome of the pathology on the polyps, she recommended a follow-up colonoscopy in three years. Yippee!
Time will tell if the sigmoid colon polyp removal and APC did the trick to stop the blood in my stools (hopefully, there are no new side effects from the APC). I guess time will tell on both counts.
Next up: Get through the holidays and PSA test sometime in late January.
Happy Thanksgiving! (I’ll get a 0/9 score after Thanksgiving dinner. 🤣)
Header Image: San Diego, California skyline at dusk.