

So it’s been 84 months since my radical prostatectomy. How am I doing?
Status
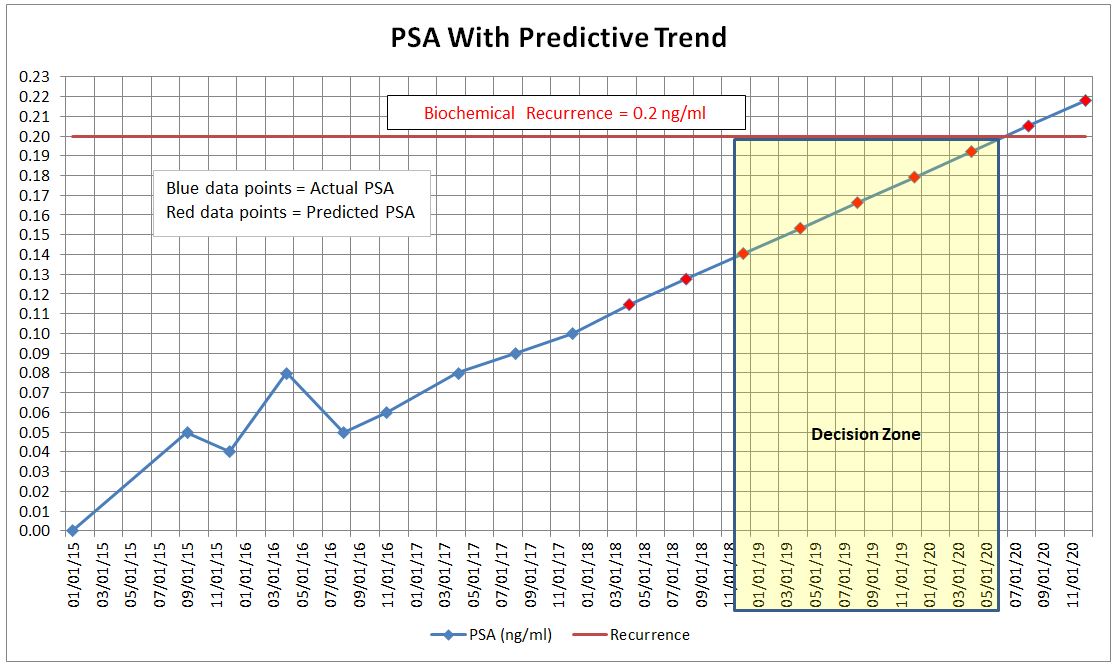
With my PSA increasing steadily over the last two years to the point where it’s now at 0.10 ng/ml, it appears that I’m on the path to recurrence. Needless to say, that’s not the outcome that I had in mind when I started this journey, but my surgeon did warn that approximately 20% of prostatectomy patients have the cancer return.
Emotions
My visit to the doctor in December went just as I expected it would, with one exception. I left the office feeling as though the wind had been knocked out of me. This whole notion of recurrence took on a whole new meaning when the doctor suggested that we’re going to have to start thinking about radiation in the future. It’s becoming real again. Since then, I’ve been doing okay. Not great. Not horrible. Okay.
Incontinence
I remain “dry” 98% of the time. There have been a few very long days at work where my body tired and, combined with the physical exertion at the end of the day, I was a bit more prone to leak. Rarely do I need to get up to go to the bathroom in the middle of the night—I can last 6-7 hours most nights.
Sexual Function
I continue to do so-so in the ED department. Remember, I have only one nerve bundle remaining, but I can get an 80%–90% erection most of the time. Some days are better; others are worse.
I do find that my libido is still there, and there are times through the day where I can feel things stirring down below. Not enough to obtain a natural erection—those days are gone—but enough that with a little stimulation, it would be much easier to achieve an erection.
Summary
Recurrence is the fear of every cancer patient because now your options become more limited and the costs of dealing with it—emotional, physical, and financial—begin to increase significantly. It’s time that I start seriously preparing for the trip down this fork in the road. The good news is that I have time with my PSA doubling time as long as it is.














{kind=link}