I came across this fact sheet on hormone therapy from the National Cancer Institute that does a great job of explaining it all to the uninitiated.
https://www.cancer.gov/types/prostate/prostate-hormone-therapy-fact-sheet


I came across this fact sheet on hormone therapy from the National Cancer Institute that does a great job of explaining it all to the uninitiated.
https://www.cancer.gov/types/prostate/prostate-hormone-therapy-fact-sheet
A moderator on the HealthUnlocked website shared a link to the new 2024 American Urological Association guidelines for salvage therapy for recurrent prostate cancer:
https://www.auanet.org/guidelines-and-quality/guidelines/salvage-therapy-for-prostate-cancer
These are the generally agreed-upon guidelines that practitioners should follow when a patient has recurrent prostate cancer after initial treatment.
Here’s another informative video about hormone therapy from the Prostate Cancer Research Institute. It answered some of the questions that I had from the previous video. Specifically:
Another timely video from the Prostate Cancer Research Institute talking about the recent EMBARK study that examines combination ADT + enzalutamide therapy versus Lupron alone or enzalutamide alone. (The study was funded by Pfizer and Astellas Pharma, the manufacturers of enzalutamide.)
There were 1,068 patients divided into three groups that were followed for five years. The groups were combination therapy (leuprolide + enzalutamide); leuprolide alone; and enzalutamide alone. The metastasis-free survival rate for each group:
One thing the study summary doesn’t address is whether combination therapy accelerates or delays the cancer developing a resistance to ADT. That would be interesting to know. While it doesn’t explicitly say in the summary, it appears that the patients were on the treatments continuously for the five years.
This is something that’s been added to my list of discussion points for my visit with the medical oncologist on 19 March.
Here’s another timely (for me) and educational video from Dr. Scholz and the Prostate Cancer Research Institute.
I have an appointment with the medical oncologist on 19 March, and this has given me a good foundation for the discussion.

Today’s meeting with the urologist went about as I expected it would. In a nutshell, we agreed to punt for another three months and see where we’re at with a new PSA test at that time.
We talked about the clean PSMA PET scan results and the fact that we remain in this inconclusive gray area right now that doesn’t bode well for making decisions about the next steps. He did suggest that I could start ADT now if I wanted to do so, and he debated about whether it would be appropriate to start ADT with abiraterone. He leaned toward just starting without abiraterone if ADT is what I wanted to do, but I also sensed that he felt no need to rush into this given the negative scan results.
One interesting comment that he made (and I wish I had taken better notes) was along the lines of ADT alone has not been shown to extend life expectancy. The unsaid implication was, “Why go through the side effects of ADT now if studies show there’s no discernable difference in the outcome?” That’s something that I need to dig into a little more.
One interesting thing that’s popped up in my conversations with others in prostate cancer forums or here is testosterone level testing. In all my years of being treated, my testosterone level has never been tested, so we talked about that. It’s something that we can do just prior to starting ADT to establish a baseline reference point.
I mentioned my email conversation with the radiation oncologist, and talked about the possibility of zapping a lesion should it show up on a PSMA PET scan in the future. The urologist seemed a bit indifferent to that approach (probably an occupational hazard).
During the conversation, I mentioned that my PSA doubling time using the last four values was at just over six months, and he commented that that was “not insignificant.”
We did discuss whether there was value in knowing where the cancer was located at this point, or to just know that the cancer is somewhere and proceed with systemic treatment without knowing its location. My concern is that starting ADT would make finding the location next to impossible on a PSMA PET scan if my PSA is knocked down to near zero.
He kept using the term “metastatic” throughout the conversation which, I suppose, is technically correct. If the cancer is someplace other than where it started, it’s metastatic. But I’ve also learned that there is a lot of gray area in the prostate cancer world when it comes to classifying how and what your cancer is.
I also asked for a consult with a medical oncologist to get his/her insights on where I’m at and what should be done next and he was going to put that request in for the consult.
I have a three-month follow-up appointment and PSA test scheduled for 14 May 2024, so the saga continues.
About an hour after I returned home from my appointment, the PCRI posted this very timely video on micro-metastatic prostate cancer.
I’ll probably publish this video as a stand-alone post so it’s easier to find.
Header Image: La Jolla Shoreline, La Jolla, California
No evidence of recurrent prostate cancer or metastatic disease.
I know I should be excited but, at the same time, I don’t think I’ve been so frustrated by “good” news. Thanks to the steady increase in my PSA, we know something is happening somewhere, and I was really hoping this scan would end the game of cat-and-mouse that we’ve been playing trying to determine where the cancer is and what to do next. It didn’t.
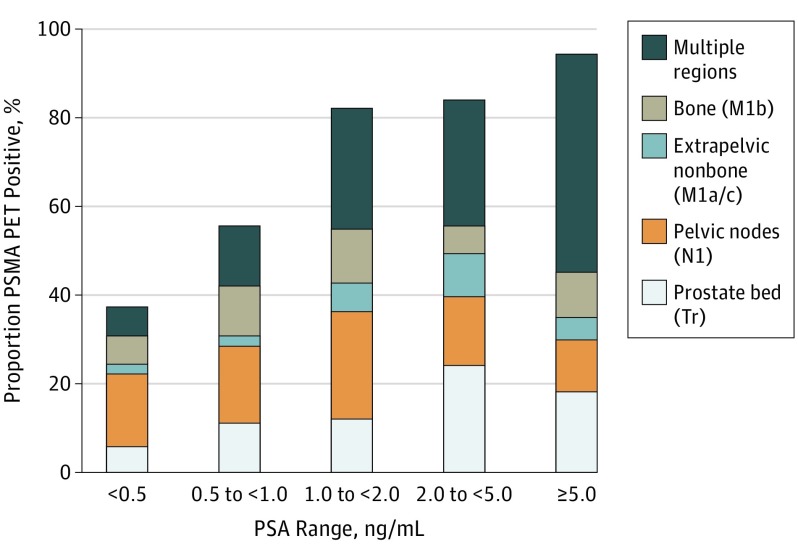
Even though I recognized going into the scan that, at my PSA level (0.37 ng/mL), there was an approximate 40% chance of detecting something, I was hopeful it would come up with something this time. Silly me and my expectations.
The other thing I’m beginning to wonder is if I’m in that 10% of patients for whom PSMA PET scans don’t work. (You may recall that being mentioned in this video from the PCRI: Rising PSA After Prostatectomy.) I have to dig into that more to see if it’s just PSMA PET scans that use Gallium-68 as the tracer, or if that applies to any PSMA PET scan regardless of the tracer used. I’m guessing it’s the latter.
Choline and Axumin scans are another option, but they don’t start reliably picking up cancer locations until the PSA is at 1.0 ng/mL or higher. Assuming my current PSA doubling time (6.2 months) remains steady, that means waiting another 11 months before I hit 1.0 ng/mL for those scans to have a chance of seeing anything.
I’ll be putting together my list of questions for the urologist appointment on 13 February (I’m open to suggestions). I suspect we’ll have a good discussion on subsequent PSA testing, the value of knowing where the cancer is located at this point, and when to start hormone therapy.
Again, the silver lining in this is that my scan didn’t light up like the Las Vegas strip. I need to keep that in mind.
Happy Friday!

PSMA PET scan No. 2 is behind me.
This was different from and easier than the first one. That’s because the VA just did a PET scan today, whereas my scan at UCLA included a CT scan on top of the PET scan.
That fact really didn’t occur to me until all was said and done. I’ll have to ask the doctor about the đifferent approaches.
In any case, today they juiced me up with Gallium-68 shortly after arrival. About 45 minutes later, I was on the scanner table ready to go. I barely felt the table move me through the scanner, and it took about 45 minutes to complete the scan.
Of course, the technician wouldn’t give me any sneak peak insights. “The doctor will interpret the scan.” I expect it could take a week or so for me to see any notes in my online records.
Again, even with my PSA closing in on 0.40 ng/mL, there’s only about a 50-50 chance it will give us any useful information at that PSA level. (As a refresher, my PSA going into the UCLA scan was 0.22 ng/mL.)
More to come.

Okay. I got antsy and went for my PSA test on Friday instead of next week. As expected, my PSA increased from 0.33 ng/mL on 6 December 2023 to 0.37 ng/mL on 19 January 2024.
The silver lining in that cloud is that the rate of increase slowed a bit and it didn’t increase as much as I expected it would.

Sometimes, I get too nerdy for my own good. There was a 91% increase between the May and October readings, and there was a 57% increase between the October and December readings, so I averaged the two increases (74%) and projected that this increase would land me at just over 0.5 ng/mL. This increase ended up being just 12% over the previous December reading. Fickle PSA.
I ran the numbers through the Memorial Sloan-Kettering PSA Doubling Time calculator again, using the five values from March 2023 (0.13) on. My PSA doubling time dropped from 6.7 months to 6.2 months, and my PSA velocity increased from 0.2 ng/mL/yr to 0.3 ng/mL/yr since calculating it back in December.
I went for the test early because I really wanted to know the PSA value going into the PSMA PET scan that’s scheduled on 31 January 2024. Plus, if it dropped, I would have had time to ask the urologist if it was worth going ahead with the scan at a lower PSA level. (Remember, I went for a PSMA PET scan when my PSA was 0.22 ng/mL, and it didn’t show anything at that PSA level. Why subject myself to another dose of Gallium-68 if the outcome may not produce any useful information?)
My follow-up with the urologist to review the PSMA PET scan and PSA results is on 13 February, and we’ll map out what’s next from there.
So that’s the latest and greatest. More to come.
Header image: The famous Torrey Pines Golf Course, San Diego, California, home to the Farmers Insurance Open golf tournament
With androgen deprivation therapy (ADT) a near certainty in my future, I’ve been trying to get smarter about it. In my research, I came across this video from Dr. Eric Small at the University of California San Francisco (UCSF), that gives an introductory overview of ADT.
If you’re not familiar with some of the lingo and drug names, it may be like taking a sip of water from a fire hose, but Dr. Small gets the concepts across pretty clearly.
After watching the video, my pea-sized brain came up with what may be an oversimplified, imperfect analogy that may make Dr. Small cringe. (I’m happy to be corrected if this analogy is out to lunch!)
We know that prostate cancer needs testosterone to survive and grow, and the testes and adrenal glands both produce testosterone. So how do we cut off the supply of testosterone from those two sources to the cancer cells?
Imagine that the cancer is your backyard swimming pool (even a kiddie pool). Pools (cancer cells) need water (testosterone) to do what they do best. Your testes are one hose that fills the pool, and your adrenal glands are the second hose that fills the pool.
If we don’t want water (testosterone) in the pool (cancer), we shut off the spigots on the hoses to stop the flow. To turn off the spigot from the testes, we use one set of drugs (Lupron, Eligard, Zoladex, Firmagon, or Orgovyx). To turn off the spigot from the adrenal glands, we use a different drug, Abiraterone.
But there’s another way to stop the pool from getting water, and that’s to place a watertight cover over the top of it. That’s what the antiandrogen drugs do—they cover the pool and stop the water from getting in. These drugs are Flutamide, Nilutamide, Bicalutamide, Enzalutamide, Apalutamide, or Darolutamide.
ADT blocks the production of testosterone and antiandrogen drugs prevent the cancer cells from receiving the testosterone.
I’m sure more research is in my future, and I’ll be certain to share what I learn. In the meantime, don’t giggle too much at my analogy.
