This video was released today, and the timing could not have been more perfect. Dr. Scholz does make the distinction between the Axumin and PSMA PET scans, confirming that the PSMA PET is more likely to pick up my cancer’s location at my PSA level.


This video was released today, and the timing could not have been more perfect. Dr. Scholz does make the distinction between the Axumin and PSMA PET scans, confirming that the PSMA PET is more likely to pick up my cancer’s location at my PSA level.
As a baby boomer, I grew up with Spock. Both of them.
First, there was Dr. Benjamin Spock, the noted pediatrician who told my parents—and millions of other parents—how to raise and care for their kids. Then, of course, there was the Star Trek Spock, whose existence was rooted in Vulcan logic.
Now I’m not a Trekkie, but if you’ve read any part of this blog, you do know that facts, figures, and logic are high on my priority list, too. I thought, “What better way is there to outline the possible scenarios and decisions that are ahead of me than to put them all in a flow chart.” So here goes:
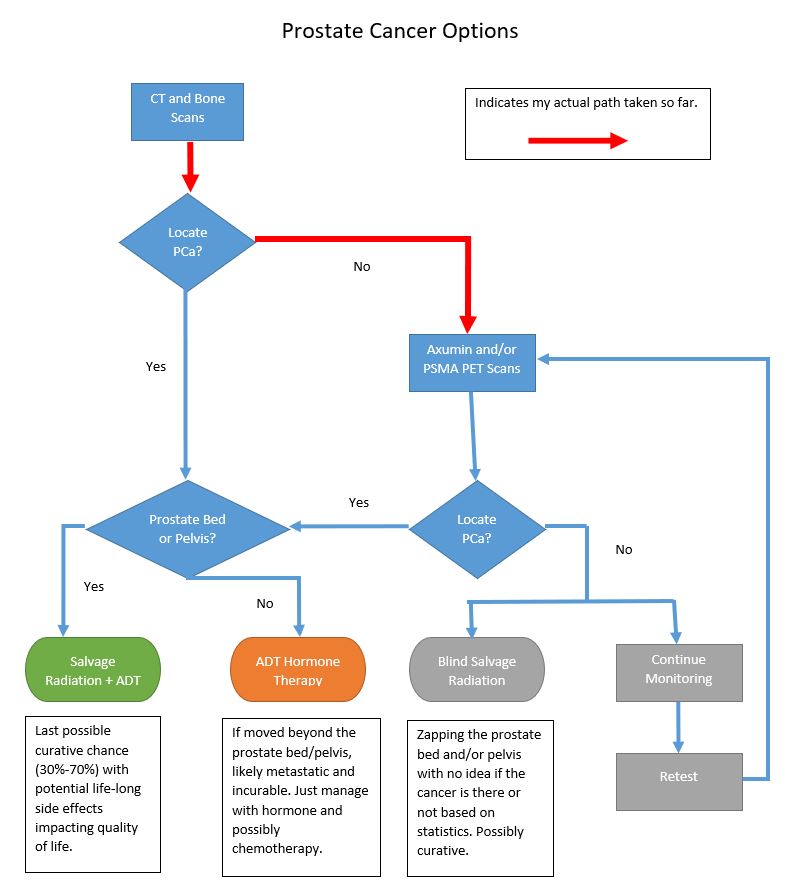
So let’s step through this.
We start with the CT and Bone scans that happened over the last two weeks. The first question is, “Did those scans determine the location of the prostate cancer (PCa)?”
If the answer is yes, then the next question is, “Was the prostate cancer in the prostate bed and/or pelvis?”
If the answer is yes, the PCa is in the prostate bed and/or pelvis, then Salvage Radiation Therapy (SRT) with or without Androgen Deprivation Therapy (ADT) (Hormone therapy) offers the last possible chance of a true cure. Of course, there are risks associated with SRT that would impact your daily quality of life: bowel control, bladder control, and lack of sexual function. Additionally, depending on which study you look at, SRT may be successful only 30% to 70% of the time. (Green bubble above.)
But if the answer is no, the PCa is outside of the prostate bed and pelvis, that means the PCa is now distant and likely metastasized. If that’s the case, there is no cure and the PCa can only be managed with hormone therapy and perhaps chemotherapy. (Orange bubble above.)
We’ve talked at some length that neither the CT scan nor the bone scan have the sensitivity to pick up the cancer’s location based on my PSA level of 0.21 ng/mL. It was very likely that neither would pick up the cancer at that first decision point on the flow chart, so further investigation is required by using the Axumin or PSMA PET scan.
In fact, neither the CT nor the bone scan picked up the location of the cancer:
No definite scintigraphic evidence of metastatic bone disease and no evidence of a widespread osseous process
So that’s actually good news with the bone scan. It shows that it has not metastasized to the bones, which is definitely a good thing. (Or, at least if there is metastasis to the bones, it’s at a level that’s unable to be picked up by the sensitivity of the scan.)
We follow my red arrows above and run the Axumin or PSMA PET scans (or both) to see if either of those can pick up the location of the cancer. I’ll have that discussion with the urologist on 3 August 2021, and we’ll see when we can get them on the calendar.
If the Axumin and/or PSMA find the cancer in the prostate bed/pelvis, then we go back to the section above and land on SRT as the option. But if it’s found outside the prostate bed/pelvis, then we go back to the other section where we just manage with ADT. (If the lesion outside the pelvis is well-defined, it may be something that could be zapped in its location. Something to explore.)
If the Axumin or PSMA PET scan cannot locate the PCa, then things get fuzzy fast.
Sure, we could go ahead and blindly complete the salvage radiation therapy, hoping that we’re zapping in the correct place. Or, we could continue to monitor for a while longer and then retest to see if the cancer can be pinpointed.
This may have been a bit of an oversimplification of what’s ahead for me, but I’m hoping that it makes sense to you.
Be well!
Today was the day for my bone scan, with two appointments to make it all happen.
I had a 10:15 a.m. appointment to get the radioactive juice (oops, contrast) injected into my system so that it had time for the scheduled 1:45 p.m. scan.
I’ve learned over the years that you have to have a little fun with those sticking needles into your arm, so I asked the nuclear medicine technician, “Has anyone ever started belting out Debbie Boone’s You Light Up My Life as you inject this stuff?”
He looked perplexed, but was old enough to know the song I was referring to.
“Uh, nope. You would be the first.”
“There’s no way I’m singing. I clear dogs from a three county radius when I do.”
He chuckled, turned the valve on my IV, and let the juice “light me up.”
The cool thing was that I checked in at the front desk at 9:50 a.m. and was walking out of there at 10:15 a.m., the time of my appointment. All done.
As I was leaving the morning appointment, the tech told me to drink plenty of fluids, and to come back at 12:45 p.m. instead of 1:45 p.m. Not a problem.
As we walked back to the scanner, he said, “Let’s get some pictures.”
“Oh. Just like my high school yearbook, except those were taken using a Daguerreotype camera.”
Without skipping a beat, he chimed in, “By Matthew Brady?”
Of course, being a native Illinoisan with an affinity for all things Abraham Lincoln and, to a lesser extent, the American Civil War, that resonated with me. [For my international readers, Matthew Brady was a photographer who pioneered photojournalism during the Civil War, and took a number of portraits of President Abraham Lincoln.]
That caused me to relay a story of when I was working at the San Diego Natural History Museum, and, when a kid learned I was from Illinois, he asked, in all earnestness, “Did you go to school with Abraham Lincoln.” Ouch!

As far as the scan was concerned, it went well. Strap me in, slide me in, and poof, we’re done in about 45 minutes or so (I never really looked at the clock to time it). But he did want to get a second run of my pelvic region. Apparently, my bladder filled with radioactive juice and he didn’t have a clear image of what was going on. After a quick trip to empty my bladder, we got a much better view.
Of course, I had to ask, “Did you see anything like Petco Park lit up at night?” [Petco Park is the baseball stadium for the San Diego Padres professional baseball team.]
He reluctantly deferred to waiting for the doctor’s interpretation, but then he offered, “I didn’t see anything.”
“Good. I won’t hold you to that,” I said.
I’ll start looking for the results online over the weekend and will post when I read them.
Have a great weekend and be well!
It’s been a week since I submitted the form on the UCLA website for a referral for the PSMA PET scan, and I hadn’t heard anything back, so I called them this morning.
When I mentioned that I submitted the form about a week ago, the agent said, “Oh. Yeah. We can’t book appointments using the form on our website. We need to take that down.” Uh. Okay. Good to know.
To schedule the PSMA scan:
They are currently scheduling appointments in September, so there’s a bit of a delay which isn’t all that surprising.
Now all I have to do is convince my doctor at the VA to go through the process once we get the bone scan results back. I’m not sure how that will go, but you can bet I’ll push pretty hard to make it happen.
If they insist on doing the Axumin scan at the VA first, I guess I’m okay with that. But if that comes back negative, I’ll really press for the PSMA PET scan. I’m just not all that keen on having all this radioactive juice injected in me over the course of a few weeks.
We’ll see how things go.
Be well!
Between work and dealing with this recurrence, I’ve been burning the candle at both ends, and it’s beginning to take its toll on me.
Don’t get me wrong, emotionally I’m doing fine. It’s just one of those periods where the further you go, the behinder you get. But I have managed to work in a little R&R along the way.
Here are just some general updates on some of things in the works:
I’m actually a bit surprised that I have yet to hear from the Nuclear Radiation department at UCLA concerning the PSMA PET scan. I submitted the online form requesting a consultation / appointment about a week ago, and crickets. I’ll give it another day or two, and then I’ll call rather than resubmit the form. Maybe I’ll get a little further that way.
One of the perks of having your office in a hospital is that you get access to people and information that you may not otherwise have.
Regular readers may recall that one of our radiation oncologists (RO) at the hospital popped into my office looking for some information. We chatted and, long story short, we had a little consult about my case right in the lobby of my office. Several months later, we ran into each other again, and we did a mini update consult.
If these CT and bone scans yield something positive, the San Diego VA Medical Center in La Jolla may very well refer me to this RO for treatment. That made me wonder: Is Dr. RO familiar enough with a Ga-68 PSMA PET scan that he would know what to do with the results?
So I asked him in an email:
I guess my question to you is how helpful to you as an RO would a PSMA PET scan be in planning SRT? I ask because VAMC San Diego once referred me here to talk with Dr. W. here at NMCSD a few years back, and I suspect that if I did get a PSMA PET scan at UCLA, VAMC would likely refer me back to NMCSD for SRT. Because it’s so new, I’m just curious if it’s been folded into your treatment planning bag of tricks.
That may have seemed pretty ballsy of me to do, but his response verified it was worth asking the question.
In short, he’s never ordered a PSMA PET scan yet and isn’t familiar with the specifics. He is, however, familiar with the Axumin scan (we have it at our hospital) but he also recognized its weakness when it comes to detecting anything at my PSA level.
Needless to say, I was quite appreciative of the fact that he took the time to answer, and to have an answer that was so open and honest. Kudos to him.
My bone scan is scheduled for Friday. I’ll pop into the lab in the morning, get my glow-in-the-dark juice injected, and then wait for about 3 hours to get scanned.
I had a baseline bone scan seven or eight years ago, and I don’t recall having any issues with the contrast for it like I did for the CT scan last week. That was awful.
Again, I don’t expect it to show much of anything, other than perhaps some further degeneration of some old injuries. But if it, on the off chance, does pop positive for distant bone metastases, that’s a whole new ballgame.
To push aside some of the stress of the last few weeks, some coworker friends of mine decided it would be a good idea for all of us to go to Tijuana, Mexico on Friday night.
It was.
Even though the border is 7 miles / 11 km from my house, this was my first trip to Tijuana since being stationed here in the Navy in 1987-1989. Let’s just say, it’s changed.
We went to a place called The Park, which is best described as a high-end food court. You’re seated at your table and a server comes to take your order from one (or more) of any of the 8 or so restaurants in the complex. When the food is ready, they’ll bring it to you. It’s an interesting concept and the food was high quality. (I have a not-so-good track record of going to Mexico and coming back with a case of Montezuma’s Revenge. Not a problem at all this time.
I have to admit that it was a bit funny, though. It was like one of those “Which one doesn’t belong” cartoons for kids. Out of the 8 of us who went, 6 were of Mexican ancestry, and 2 of us weren’t. Can you say, “Odd man out?”
Look for the write-up coming out soon on my other website, ExploreSanDiegoandBeyond.com.
Lastly, I have my appointment with the urologist to review the CT and bone scan results on 3 August 2021. I hope to have some answers from UCLA by then so we can have the Axumin vs. PSMA PET scan discussion in earnest, and figure out which one we’ll pursue next.
So that’s it. Just a lot of administrative stuff, testing, waiting, and more of the same.
I’ll keep you posted on how things progress. Perhaps from a bar in Tijuana.
Be well!
Let’s start with the BLUF:
No definite evidence of locally recurrent or metastatic disease within the abdomen or pelvis.
(If you don’t know, BLUF = Bottom Line Up Front).
There was one 9 mm kidney-shaped lymph node that caught their attention, but didn’t think it to be remarkable.
They also commented on a bunch of my other organs and bits and pieces, but nothing seemed too out of the ordinary for any of them aside from a few dents and scratches from 63+ years of normal wear-and-tear and countless miles/kilometers.
The fact that the CT scan didn’t pick anything of substance up is a good thing and a bad thing. Good because it didn’t see anything; bad because it didn’t see anything. The likelihood of it detecting the lesions at my PSA level were small, and we knew that going into this. So even though we didn’t see anything, that doesn’t necessarily mean that it’s not there.
I did get a chuckle out of one line in the report:
Multidetector CT abdomen/pelvis was obtained after the uneventful administration of intravenous contrast.
Uneventful for who??? The radiologist? Sure. I did everything in my power to not puke all over their $300,000 scanner. 😲
I expect we’ll have the same result with bone scan next week, but time will tell.
That’s all for now.
Be well!
Just a quick update…
This morning, I went onto the UCLA website and filled out the form to request more information about the Ga68 PSMA PET scan and perhaps even schedule an appointment with them. We’ll see how long it takes for them to respond. I’m gue$$ing it may be pretty quickly as they want to get more people using their test and facility. Ju$t a hun¢h.
“Cynic, table for one. Cynic.”
That contrast used in the CT scan yesterday really kicked my butt. The juice was injected into me shortly after 2 p.m., and as I was heading to bed around 9 p.m., I could still feel some of the side effects from it.
I did drink a lot of liquids to help purge it from my system and that translated into multiple runs to the toilet through the night last night. Oh well. It all caught up with me around 2 p.m. this afternoon when my ability to focus just ran head-on into a brick wall. I hung it up at the office and came home.
I just checked for the scan results online, and nothing posted yet. I suspect it will be on the weekend that I’ll be able to see them. Of course, they’re usually written in such a away that a lay person has trouble comprehending what’s on the page. We’ll give it a try, though, when the time comes.
That’s about it for today. Hopefully, the next post has news about the PSMA test or the CT scan results, or both.
Until then, be well!
Congrats to Jim P.!!!
You’re the person who gave the 1,000th like on my blog!

I wish I could give you a prize like a trip to your dream destination or a cure for this pesky disease but, alas, I don’t have a magic wand to make either happen.
But to everyone who’s followed along and liked the content, thank you!
Be well!
You know me. I love tracking things, and this post is the 400th published post on this blog. Woo-hoo! 🎈🎉✨ Of course, I would have preferred to not have written any of them at all, but that’s life.
I thought I had had a CT scan in the past, but if I did, I don’t remember it being anything like what I experienced today. It kicked my ass. Technically, it was the contrast they injected into me that kicked my ass. The scan—sliding in and out of the scanner—was a non-event.
The radiologist forewarned me of the sensations that I would experience shortly after he injected the contrast. The sensation of a full and warm bladder? Check. Metallic taste in my mouth? Check. A warm sensation throughout my body? Check.
What he didn’t do a very good job of was forewarning me of the intensity of the some of these things. At one point, I thought I was going to vomit like Vesuvius. It was awful. As soon as he stopped the IV flow of contrast, I could feel some of these side effects dissipating. (But not nearly as quickly as they came on.)
I didn’t even bother to ask the technician if they saw anything odd on the scan as they were running the test. I’ll usually do that because sometimes, if you’re lucky, the technician will help you out. They may not be able to be all that specific, but I’ve had one or two tell me, “You really don’t have anything to worry about.” I was just more focused on getting out of there without puking.
The whole appointment went like clockwork and went faster than I expected. My appointment was for 2:30 p.m. I pulled into the parking garage at 1:45 p.m.; was checked in a Radiology by 2 p.m.; on the scanner bed by 2:10 p.m.; and headed back to my car by 2:35 p.m. Again, I know there are tons of complaints about the VA healthcare system, but San Diego VA Medical Center has been top-notch as far as I’m concerned.
The radiologist thought they would have the full results available by Friday.
I’ll have to admit that on my commute to work this morning, I had a bit of a knot in my stomach. Not because I was afraid of the scan (now I am—a little), but because this is the beginning of the process that will give me results I may not want to hear.
On a related note, my employer-provided healthcare insurance did confirm that the Department of Nuclear Medicine at UCLA is in network, so that’s a good thing.
What’s next? Here’s an estimated timeline:
I’ll contact UCLA to start that process and hopefully have all of my homework done in time for the appointment on 3 August.
Well, time to drink a few liters of water to purge that contrast out of me.
Be well!
“It’s been a quiet week in Lake Wobegon, my hometown…”
Yeah, right.
There’s really nothing new to report regarding the PSMA PET scan and insurance coverage. I’m still awaiting explicit clarification that I will be covered and that UCLA is in-network. More to come.
What I do want to talk about in this month’s post is some of the resources that I routinely use to do my research on all of this. There are a few that I believe have high quality, easy-to-understand information for patients, and there are a few that keep you informed of the latest research and treatment options.
As you’ve seen in a few of my recent posts, I’ve been a little late to the game in terms of finding some very educational YouTube videos that talk about prostate cancer and treatment options. I may create playlists of videos that I’ve saved on the YouTube account associated with my contact information.
The Prostate Cancer Research Institute is a wealth of information that’s presented in such a way that patients and their partners can easily understand. My only criticism is their color-coded staging system that they use. I believe they created it thinking it would simplify things, but it’s not used beyond PCRI (as far as I can tell), so it can be quite foreign initially.
PCRI’s videos are short and packed with information. They also answer a number of the more common viewers’ questions left in the comments.
Lastly, they do have a patient helpline that you can access either online or via phone. They were pretty timely in their response to an online question that I submitted.
The New Prostate Cancer Infolink is a great source of information regarding current research on a variety of prostate cancer-related topics. The website isn’t the most aesthetically pleasing, but there is a wealth of current information available. Some of it is a bit on the technical side, but most of the posts include links to the specific research articles they mention. That can be handy if you’re the type of person who likes to read that stuff. (Hmmm… Remind you of anyone in particular???)
I’ve found that the authors are generally responsive to comments or questions left on the post.
You can check out the Resources page on my blog to learn about a number of other resources. Some are quite general in their approach to educating patients, some are a bit more specific, and, sadly(?), some to be more focused on fundraising than patient education. Don’t get me wrong, Funding research is critically important. It’s just that you may not find some of the detailed information you’re seeking on those sites.
The other thing that’s interesting is how each major organization interprets the same topic and provides oftentimes differing information between organizations. Welcome to the frustration of prostate cancer research. I tend to look for the commonality between the information being shared, and that tends to reinforce that it’s a more widely accepted approach.
Lastly, I always look at the “freshness” of the articles or papers that I’m reading. Were the written in 2020, or in 1997? That can make a significant difference, too. When you’re looking at retrospective studies that tracked patients for 7, 10, 15, or more years, you have to remember that treatment technologies and methods have changed in those periods of time. So the statistics you’ll see in the report may be slightly biased because of their age and the changes in the field of prostate cancer management.
Of course, always be wary of prostate cancer blogs written by crazy, bitter old men sitting around in their underwear on their computers… Be especially wary of #13 and #26 on this list. 😂
Yes, researching prostate cancer can be absolutely maddening but, if you do it correctly, it will pay off in the end. It makes you a much better educated patient, and you can have far more credibility and influence with your medical team than if you’re just along for the ride. And if you think the doctors don’t notice, they do. Here’s my doctor’s notes from my last visit:
Very well informed about his disease. Uses MSK nomogram.
He brings an article regarding68Ga-PSMA 11 PET scan. He
reports that if PSA is truly at 0.21 that he would like to
complete, even if he needs to pay out of pocket.
He is involved with support groups and has a blog Dansjourney.com
I was a little disappointed, however, that there was no ⭐. 😂🤣😂
Okay. Enough silliness. Time to put my pants on, step away from the keyboard, and enjoy the 75° F / 24° C San Diego day.
Be well!
