I went for my PSA test Tuesday morning and came away with two surprises.
First, I was able to get my results online at 11:52 p.m., Tuesday night (yes, I’m a night owl). I’ve never had the VA turn them around that quickly before.
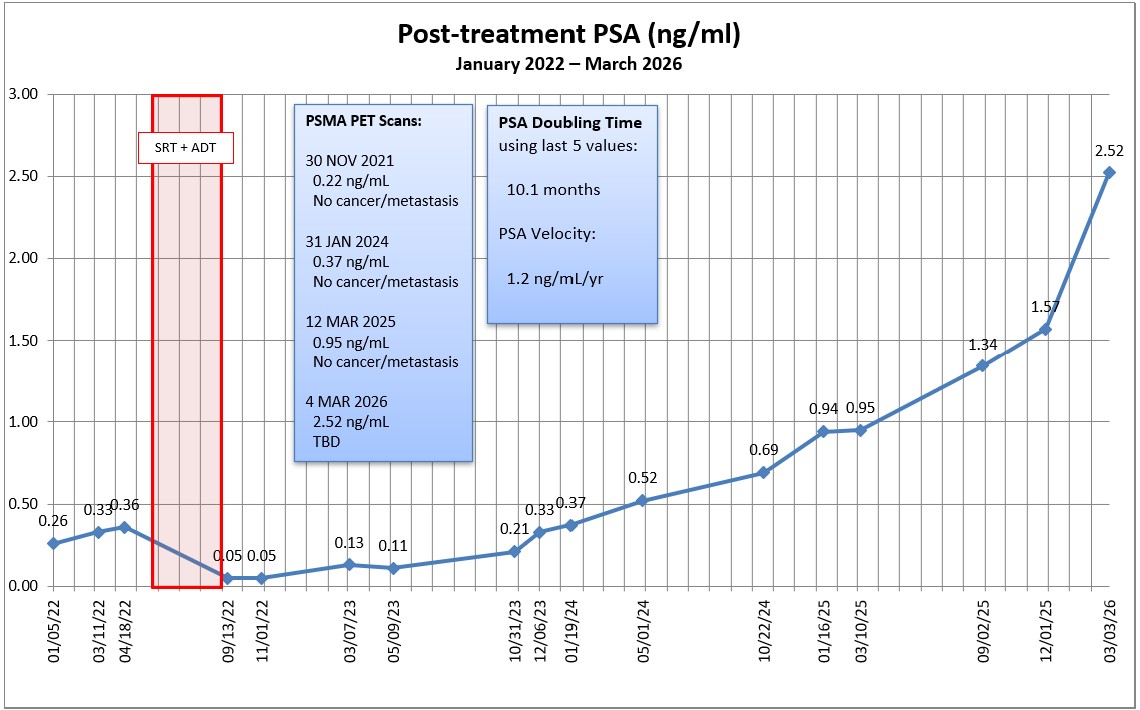
Second, my PSA jumped significantly to 2.52 ng/mL from 1.57 ng/mL on 1 December 2025. That gives a PSA doubling time of 10.1 months using the last 5 readings (back to January 2025).
I expected an increase, but not that much of an increase. On the positive (?) side, that should make finding lesions with my PSMA PET scan in 10 hours much easier. (It’s now 12:30 a.m., Wednesday as I’m typing this.)
I suspect it will take a week or so for my PSMA PET scan results to be posted, and I’ll update once I have them.
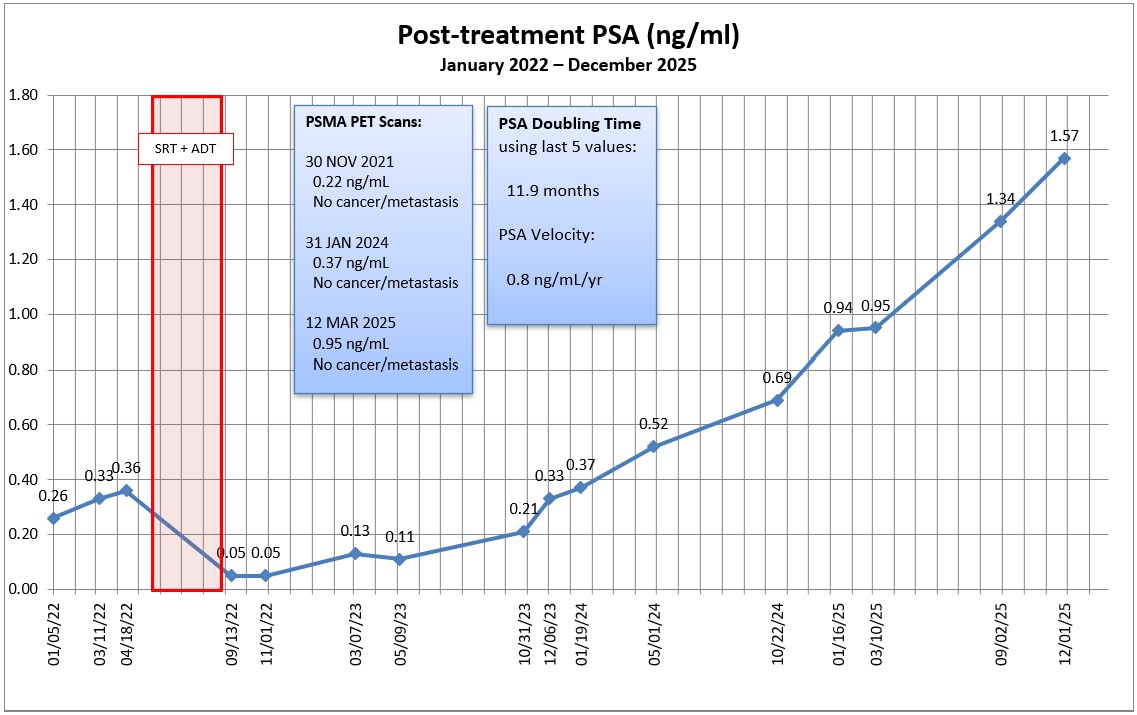
It’s that time again. My PSA came back at 1.57 ng/mL, up from 1.34 ng/mL in September.
PSA doubling time using the last five values increased slightly from 11.5 months in September to 11.9 months now. PSA Velocity went from 0.6 to 0.8 ng/mL/yr.
My appointment to review the results is on 30 December 2025, and I’ll be sure to talk about another PSMA PET scan to see if we can determine what’s going on before we start down the androgen deprivation (hormone) therapy path.
On an unrelated note, I managed to take a little drive through the country from San Diego to visit family in southeastern Wisconsin and back last month. You can check out the full story HERE if you’re bored.
In a nutshell, we’re punting the ball another three months down the road.
The doctor commented on the continuing rise in my PSA and said after consulting with the doctor who saw me last time, said that he wanted to recheck my PSA in six months and “wait a year” for another PSMA PET scan. I should have asked for clarification on that, but I think he was referring to waiting a year after my last PSMA PET scan in March 2025 and not a year from today.
I wasn’t entirely comfortable with waiting another six months, so we agreed to test PSA again in December (three months after my September test) and go from there.
We also talked about spot radiation if anything pops up on the scan. He seemed a bit reluctant for that to be an option, and went straight to starting hormone therapy. It’s as though he was making the transition from curative options to management options, and, to be perfectly honest, I believe I made that transition in my own mind once the salvage radiation failed. That doesn’t mean that I wouldn’t try zapping a lesion or two if they popped up on the scan depending on location (no more zapping to the pelvis and risking further bowel complications).
We did talk about my experience with hormone therapy during the salvage radiation, and the timing of starting it this time around. In that discussion, he brought up the topic of bringing in a medical oncologist at some point depending on the scan results and my PSA test results.
We talked at length about my urinary frequency and some options for that. He suggested some pelvic floor therapy might be beneficial, so I said I’d be willing to give that a try.
Overall, I’m okay with where we’re at and the planned course of action for now. I’ll go for my PSA test in early December, and if there’s another significant jump, I’ll press for the PSMA PET scan to be done sooner rather than later.
My next scheduled urologist appointment is 30 December 2025.
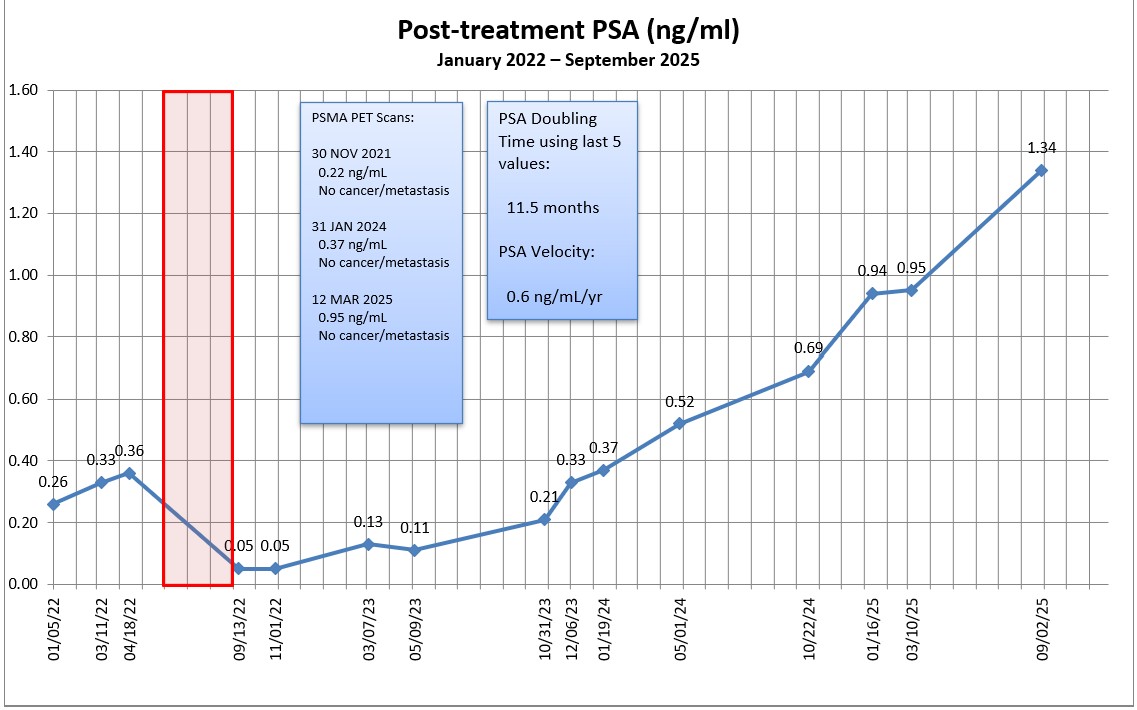
My PSA jumped 41% from 0.95 ng/mL to 1.34 ng/mL, and, interestingly, my PSA doubling time went from 10.0 months to 11.5 months using the last five readings.
Needless to say, that was a larger increase than I expected, but I’m also not surprised or panicked about it.
I’ll gather my thoughts and send an email to the urologist to seek his/her guidance. I’ll mention the canceled and rescheduled appointment; ask for their thoughts about another PSMA PET scan (or other scan); and ask, “What’s next?”
Other than that, I really don’t know what else needs to be done in this limbo period of being between one treatment and the likely next treatment.
More to follow. Be well.
Header image:Beach and Cliffs, Torrey Pines State Natural Reserve, San Diego, California
I went for my PSA blood draw this morning on the day after our Labor Day holiday weekend. I thought the clinic might be packed, but I was pleasantly surprised. It took 9 minutes from checking in at the kiosk to walking out the door.
I’m guessing that I should be able to access my results online on Friday or Saturday. The trend function on my PSA tracking spreadsheet suggests that my PSA will increase from 0.95 ng/mL back in March to 1.09 ng/mL today. We’ll see if the actual results are anywhere close.
You may recall that my last urologist appointment was on 1 April 2025, and we scheduled the six-month follow-up on 30 September. A few weeks ago, the VA canceled that September appointment and the earliest re-schedule slot was on 30 December. I haven’t called to squeal about that yet because I wanted to see what the results of the PSA test are first.
If the results go from 0.95 ng/mL to 1.0 or so—even the quasi predicted 1.09 ng/mL—it doesn’t seem that urgent and I’ll just email the urologist and have a discussion as to next steps from there. I’ll also look at any changes in PSA doubling time to help determine urgency. But if the results really jump substantially, e.g., 1.4, 1.6, 2.0, etc., then I’ll work to get that 30 December appointment moved up to a much earlier date.
I suspect another PSMA PET (or other) scan may be in my future to see if we can finally determine what’s going on inside of me.
On the whole, the news is good. My PSA just barely bumped up from 0.94 ng/mL in January to 0.95 ng/mL in March and, taking the last five readings, that increased my PSA doubling time from 7.7 months to 10 months.
The PSMA PET scan revealed “no evidence of prostate cancer or metastatic disease.”
So, if the news is good, why am I “so over this?”
I was really hoping that this third PSMA PET scan would bring some clarity as to where the cancer was located so we could know how to proceed—even if it meant revealing metastatic disease. It’s frustrating because we know the cancer is somewhere and because we know the PSA almost tripled between 19 January 2024 and 16 January 2025, but we don’t have enough information to do anything about it. It’s just more waiting in limbo.
Of course, having had three PSMA PET scans all turn up negative makes me question if I’m in that “lucky” category of ten percent of patients whose prostate cancer doesn’t express PSMA, making the scans useless for me. It’s something that I’ll definitely discuss with the doctor at my next appointment on 1 April 2025. I vaguely recall that there’s some sort of genomic test that may be able to assess if I really do fall into that ten percent. I’ll have to do some research on that.
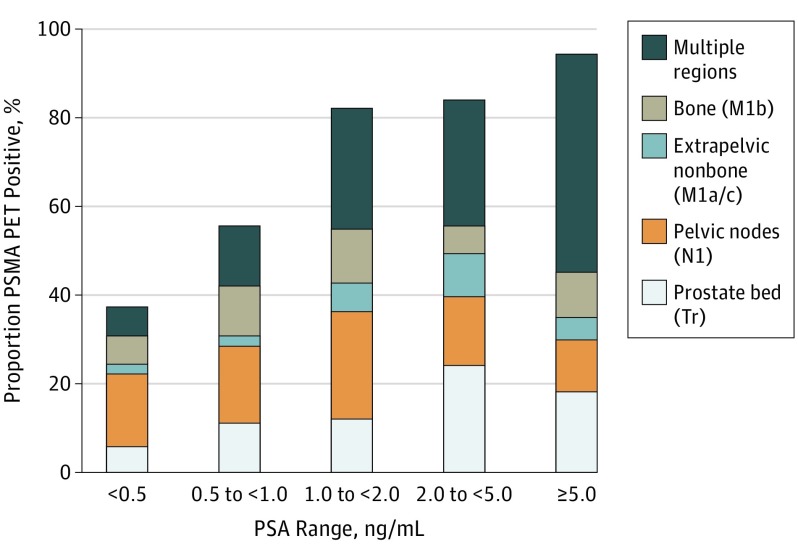
Maybe, too, I’ve placed too much faith in the scan’s ability to detect anything at my PSA level. But with a PSA level hovering around 1.0 ng/mL I thought we would have a decent chance of detecting something (chart below).
Detection Rate on a Patient Basis Stratified by PSA and Region Tr indicates prostate bed only; N1, pelvic nodes only; M1, extrapelvic only. Proportion of patients with 68Ga-PSMA-11 PET positive findings were stratified by PSA range and region of disease in accordance with PROMISE. https://pubmed.ncbi.nlm.nih.gov/30920593/
Needless to say, I’m truly glad that my PSA didn’t rocket even higher and that my scan didn’t light up like Times Square. Having definitive answers, though, would be the icing on the cake.
As far as the PSMA PET scan itself, it was pretty easy and took two hours to go through the entire process. I was instructed to drink 500 ml of water starting 2 hours before the scheduled scan time, and that was the only preparation needed.
I arrived at the hospital at 8 a.m. and was brought back to a radiation-proofed exam room where the technician started and IV at around 8:15 a.m. The 68Ga tracer was ready for injection around 8:40 a.m.
Around 9:30 a.m., the technician brought me back to the scanner where I got positioned on the bed and we began the scan which took 45 minutes. The scanner was very quiet (I could have dozed off) and large enough that it wasn’t claustrophobic. I was out of there by 10:15 a.m. and on my way home. Piece of cake.
On a related note, this was the longest it’s ever taken me to get the PSA test results posted online (hence the delay in this post). I actually called the clinic to get them over the phone because they still weren’t available online today (Thursday). The nurse I spoke with was very helpful and said, “We’re facing staffing issues and, well…” stopping herself in mid-sentence, probably remembering that the call was being recorded and not wanting to make a statement about the current environment for VA employees at the moment. I fear that this may be a precursor of things to come.
The trend formula on my Excel spreadsheet predicted that my PSA would come in at 0.69 ng/mL, and my PSA came in at exactly 0.69 ng/mL. Not too shabby.
To be honest, that’s a little better than I expected it to be, which I’m not complaining about. At least it hasn’t taken off like a Halloween bat out of Hell.
The one question that we’ll have to answer at the appointment with the urologist on 14 November is whether that level is high enough to warrant another PSMA PET scan to see if we can detect any hotspots that may be amenable to radiation. At my current PSA level, there’s about a 70% chance of detecting anything, but if we wait until the PSA is closer to 1.0 ng/mL, there’s a 90% chance of detection. Maybe we wait another three months and go from there? Or, maybe we go ahead with the scan now and I have cool images to include with my Christmas cards.
I’m guessing that that was a small enough increase—keeping my PSA at a low level—that we won’t have to worry about starting androgen deprivation therapy (ADT) quite yet. Of course, I could be wrong.
When I use my last five PSA tests over the last year to calculate PSA doubling time, the PSADT is 7.7 months.
Stay tuned.
PSA Chart since salvage radiation therapyPSA Chart since diagnosis
Header image: Anza-Borrego Desert State Park, California
I went for my PSA test this morning, so now the waiting begins for the results to be posted online. I suspect that I’ll be able to access them late Thursday night or Friday.
I also had about four or five other tubes of blood drawn (I can’t watch 🤢) for my annual physical with my primary care physician on 4 November. While there, I also got my high-dose flu shot for old geezers and the updated COVID vaccine. All of that turned me into veritable pin cushion this morning.
As much flak as the VA Healthcare system receives, I have to admit that I’m always impressed with my local clinic. No appointment was needed for either the lab work or the vaccines, and it took just 17 minutes from the time I checked in until my lab work was completed, and another seven minutes to get the vaccines. I was in and out in 24 minutes. I challenge civilian clinics to match that.
Well, it’s nearly time for the PSA roller coaster to depart the station once again. (You never get off the PSA roller coaster, you just keep riding it in never-ending loops.)
I’m not exactly sure when I’ll go to the lab—either next week (short holiday week) or the week after—but I need to get it done by the end of the month because I have an appointment with my primary care physician on 4 November, and an appointment with the urologist on 14 November. I suspect that I’ll get my seasonal flu shot while I’m at the clinic, too.
If anyone is interested, we could get a pool going to guess where the PSA test results will come in at. 😄 On 1 May 2024, it was 0.52 ng/mL. The “Trend” function on my spreadsheet has it coming in at 0.70 ng/mL using the last five PSA test results from my post-radiation nadir. My money would be on somewhere between 0.80 ng/mL and 1.0 ng/mL.
Other than that, I’m just getting ready for the palm fronds to start falling as we get deeper into autumn here in San Diego. 😂
On a fun note, I attended both of the San Diego Padres Wild Card baseball games on 1 and 2 October, and the crowd went bonkers when we clinched the best-of-three series to win a spot in the playoffs.
We’re playing our arch nemesis, the Los Angeles Dodgers, in Game 5 of the National League Division Series tonight (Friday, 11 October) to see who advances to the National League Championship Series. (We’re tied two games apiece and the winner of tonight’s game will advance. Hope I didn’t jinx ourselves by writing about this. 🤞)
Sorry for the shaky camera work. There was so much happening all over the place, it was tough to know what to focus on.
On an even funnier note, I found this perfect bed for those suffering from hot flashes while on hormone therapy.
Header image: Crepuscular rays at sunset over the Salton Sea, California while hoping to see Comet Tsuchinshan-ATLAS on 10 October 2024.(I didn’t.)
Okay. I got antsy and went for my PSA test on Friday instead of next week. As expected, my PSA increased from 0.33 ng/mL on 6 December 2023 to 0.37 ng/mL on 19 January 2024.
The silver lining in that cloud is that the rate of increase slowed a bit and it didn’t increase as much as I expected it would.
Sometimes, I get too nerdy for my own good. There was a 91% increase between the May and October readings, and there was a 57% increase between the October and December readings, so I averaged the two increases (74%) and projected that this increase would land me at just over 0.5 ng/mL. This increase ended up being just 12% over the previous December reading. Fickle PSA.
I ran the numbers through the Memorial Sloan-Kettering PSA Doubling Time calculator again, using the five values from March 2023 (0.13) on. My PSA doubling time dropped from 6.7 months to 6.2 months, and my PSA velocity increased from 0.2 ng/mL/yr to 0.3 ng/mL/yr since calculating it back in December.
I went for the test early because I really wanted to know the PSA value going into the PSMA PET scan that’s scheduled on 31 January 2024. Plus, if it dropped, I would have had time to ask the urologist if it was worth going ahead with the scan at a lower PSA level. (Remember, I went for a PSMA PET scan when my PSA was 0.22 ng/mL, and it didn’t show anything at that PSA level. Why subject myself to another dose of Gallium-68 if the outcome may not produce any useful information?)
My follow-up with the urologist to review the PSMA PET scan and PSA results is on 13 February, and we’ll map out what’s next from there.
So that’s the latest and greatest. More to come.
Header image: The famous Torrey Pines Golf Course, San Diego, California, home to the Farmers Insurance Open golf tournament