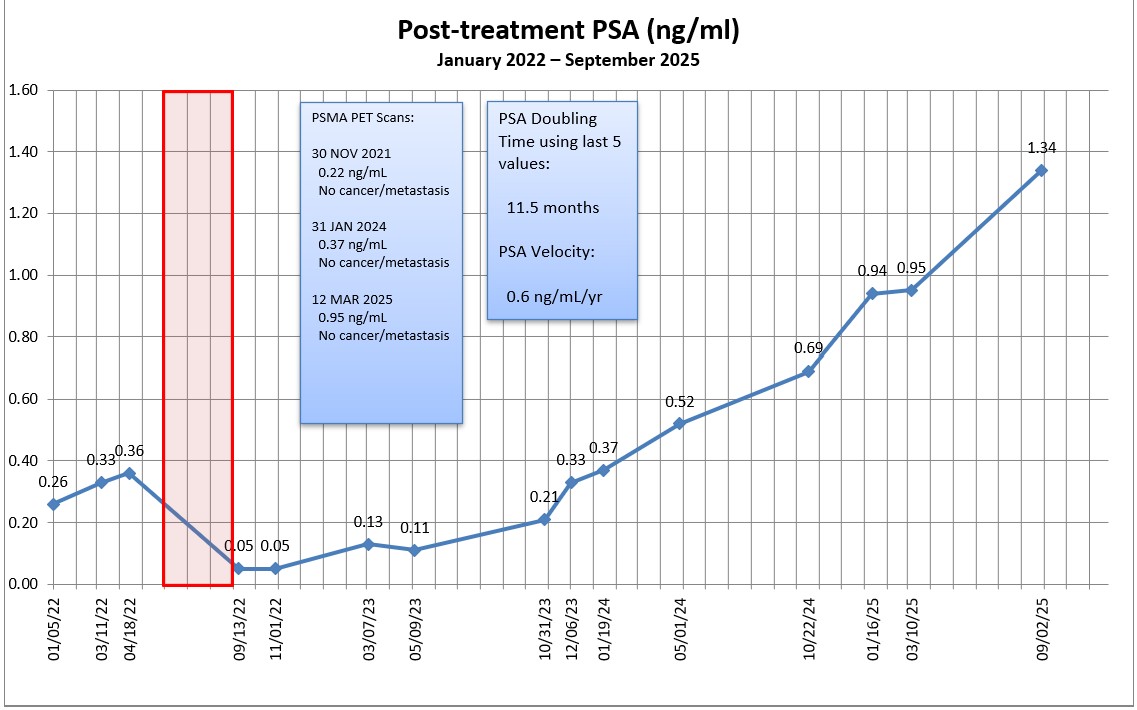
My PSA jumped 41% from 0.95 ng/mL to 1.34 ng/mL, and, interestingly, my PSA doubling time went from 10.0 months to 11.5 months using the last five readings.
Needless to say, that was a larger increase than I expected, but I’m also not surprised or panicked about it.
I’ll gather my thoughts and send an email to the urologist to seek his/her guidance. I’ll mention the canceled and rescheduled appointment; ask for their thoughts about another PSMA PET scan (or other scan); and ask, “What’s next?”
Other than that, I really don’t know what else needs to be done in this limbo period of being between one treatment and the likely next treatment.
More to follow. Be well.
Header image:Beach and Cliffs, Torrey Pines State Natural Reserve, San Diego, California
I went for my PSA blood draw this morning on the day after our Labor Day holiday weekend. I thought the clinic might be packed, but I was pleasantly surprised. It took 9 minutes from checking in at the kiosk to walking out the door.
I’m guessing that I should be able to access my results online on Friday or Saturday. The trend function on my PSA tracking spreadsheet suggests that my PSA will increase from 0.95 ng/mL back in March to 1.09 ng/mL today. We’ll see if the actual results are anywhere close.
You may recall that my last urologist appointment was on 1 April 2025, and we scheduled the six-month follow-up on 30 September. A few weeks ago, the VA canceled that September appointment and the earliest re-schedule slot was on 30 December. I haven’t called to squeal about that yet because I wanted to see what the results of the PSA test are first.
If the results go from 0.95 ng/mL to 1.0 or so—even the quasi predicted 1.09 ng/mL—it doesn’t seem that urgent and I’ll just email the urologist and have a discussion as to next steps from there. I’ll also look at any changes in PSA doubling time to help determine urgency. But if the results really jump substantially, e.g., 1.4, 1.6, 2.0, etc., then I’ll work to get that 30 December appointment moved up to a much earlier date.
I suspect another PSMA PET (or other) scan may be in my future to see if we can finally determine what’s going on inside of me.
Excuse my use of the vernacular, but I had to pee seven times through the night, and that’s a record for me.
I did what I call a preemptive pee before going to bed at 10:02 p.m., and then got up to pee again at 12:11 a.m., 1:06 a.m., 1:47 a.m., 2:48 a.m., 3:49 a.m., and 7:07 a.m.1 It’s nuts. And exhausting.
I also try to keep track of my fluid intake and to slow it down before going to bed. Monday, I joined a friend for happy hour and had two pints of beer between 4 p.m. and 6 p.m., and then had another 12-ounce can of soda at 7:40 p.m.
While Monday night’s experience isn’t typical, I have noticed a trend in that general direction since the salvage radiation therapy three years ago, and in the last few months in particular.
Because it wasn’t a huge issue, I wasn’t doing dedicating tracking, but I would say that I was going to the toilet one to three times a night, and maybe four times on a bad night. Recently, it seems it’s more like two to four times per night.
In writing the above, I was going to make the comment that I stay away from caffeinated sodas because I thought that caffeine was a diuretic. I went to confirm that via a Google search, and then went a little deeper into the rabbit hole and asked if beer was a diuretic.
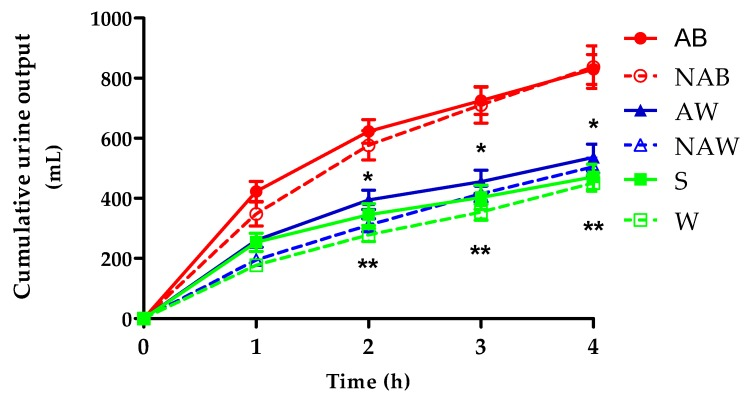
It was a small study involving 20 men that measured, among other things, urine output at four and 24 hours after drinking alcoholic and non-alcoholic versions of beer and wine; spirits; and water. The one thing that surprised me was how much cumulative urine output there was for both beer and non-alcoholic beer, especially when the test subjects were given only 250 ml of beer (a U.S. pint is 473 ml). There was essentially no difference in output between the alcoholic beer (AB) and the non-alcoholic beer (NAB).
One question that I would have for the researchers is that, if alcohol is a diuretic, why is there essentially no difference between the alcoholic and non-alcoholic beer outputs?
Needless to say, this little exercise opened my eyes and I’ll definitely consider the timing and quantity of any beer consumption going forward.
On a related note, Tuesday, I had a 16-ounce soda around 6:30 p.m. that took until 8 p.m. to finish, and I only peed 3 times through the night.
Also on a related note, it seems that my flow, while constant and steady, seems to have slightly less pressure behind it. That has me wondering if there are post-radiation strictures forming or if there may be a growth forming in the area as my PSA increases. That, or it could all be in my head. I’ll keep an eye out for changes over time.
My next appointment with the urologist was scheduled on 30 September, but I received a call from the VA this morning cancelling the appointment. I can’t recall the VA having cancelled an appointment on me at any other time during the 12 years I’ve been going there. (They have, however, called me if an earlier appointment became available.)
The scheduler said that the urology clinic would be closed for the day so that they could interview new residents. I found that interesting because I recently read an article that doctors and nurses who were extended job offers by the VA between January and March 2025 were rejecting those offers at a rate of nearly 40%, which is quadruple the rejection rate during the same period in 2024. Given the uncertainty and instability that this administration has placed on the VA with its announced cuts, medical professionals simply don’t want to risk working there.
The first available appointment for me was 30 December 2025, so I booked it.
I did confirm with scheduler that there is an order in for a PSA test, and I can go in for the lab work on or after 1 September 2025. I mentioned to her that, if the PSA results came back significantly worse, I would be writing the urology clinic and asking for an appointment much sooner.
That’s it for now. Remember, that September is Prostate Cancer Awareness Month, so please share your story with others just to educate and increase awareness.
Be well!
1 I use an app called Simple Time Tracker to record each time I pee and when I drink. I use a widget on my phone’s home screen to just tap once which makes it very easy to record the event. The app, though, is set up to measure the duration of the event, so I have to tap a second time to stop recording the duration. Of course, it has the ability to export the data to—you guessed it—a spreadsheet.
Header image: Petco Park, home of the San Diego Padres baseball team, San Diego, California
If you’ve been reading my blog for any period of time, you already know that I have a penchant for marking anniversaries or important dates. Today marks three years since I started my 35 sessions of salvage radiation therapy to deal with my recurrent prostate cancer.
I’m still here, and so is the cancer.
Interestingly, I’ve managed to quite successfully suppress my concerns about it for the last few months as I wait for my next PSA test in September. I can’t do anything about it, so why worry while I’m waiting, right?
Instead, I’ve been doing my best to maximize each day (although a few days, I’m a complete slug and don’t do much of anything—the perks of retirement!). I had a good trip back to the Midwest to visit family and friends at the end of May; have been taking a few local trips; and just chill with friends at my local watering hole. Life is good.
That all doesn’t mean that I’ve completely forgotten about the little bugs inside me. The treatment side effects remind me that it’s still there every day, but they’re tolerable.
My appointment with the urologist is on 30 September, so I’ll get my PSA test done a week or two in advance to allow time for the results to come in.
I feel as though I’m falling down in my blogging responsibilities, because I got nothin’ to report this month. However, that means that things are going well as I continue to live life with prostate cancer.
In fact, things are going so well that I treated myself to a little retirement bucket list trip to Aotearoa / New Zealand that I just returned from last week.
It was a fantastic, albeit, too short of a trip to a place that I’ve been wanting to visit and photograph for years. I’ll spare you the details here, but if you’re interested and have half an hour or so, you can check out my full trip summary (with over 100 photos and videos) here:
I had my post-PSMA PET scan visit with the urologist today, and I wasn’t really sure what to expect going into it.
The doctor (same as last time) shared the scan results saying that they’re something I should celebrate. I mentioned, though, that I have had three scans and were inconclusive despite the rising PSA numbers. He was quick to reply by saying that the scan not showing evidence of prostate cancer or metastasis was conclusive.
I understand where he’s coming from, but until we know where the cancer is, I’m going to have a difficult time accepting that perspective.
I did ask whether there was some sort of test that can determine if my cancer doesn’t express PSMA, and he said that there wasn’t. Something in my pea-sized brain tells me I need to double check him on that.
I also asked if there could be another explanation beyond the cancer that would explain my rising PSA. He ruled out the possibility of some residual prostate tissue being left behind after the surgery as being the cause based on my PSA kinetics over time.
In terms of what’s next, we’re kicking the can six months down the road for another PSA test and follow-up. I was a bit surprised that he wanted to wait six months, and suggested doing the test in three or four months. He was a bit insistent on the six month window. He felt comfortable with my current situation—the slight increase in my last PSA test from the previous one and my PSA doubling time—that waiting six months wouldn’t be a problem. He also argued that having a longer period between tests would better reflect what’s going on.
As we wrapped up, he reminded me that the scan results were good news, and I know that he’s right in that regard. I’ll work on changing my own perspective going forward (even though those little cancer bugs are still doing their thing inside me.)
My follow-up appointment is on 30 September 2025.
That’s it for today. Be well!
Header image: Cherry Blossoms, Japanese Friendship Garden, San Diego, California
In case you’re interested, the Prostate Cancer Research Institute is hosting its mid-year update tomorrow, Saturday, 29 March 2025 from 8:30 a.m. to 5:30 p.m., PDT (Los Angeles time). You can learn more about it here:
On the whole, the news is good. My PSA just barely bumped up from 0.94 ng/mL in January to 0.95 ng/mL in March and, taking the last five readings, that increased my PSA doubling time from 7.7 months to 10 months.
The PSMA PET scan revealed “no evidence of prostate cancer or metastatic disease.”
So, if the news is good, why am I “so over this?”
I was really hoping that this third PSMA PET scan would bring some clarity as to where the cancer was located so we could know how to proceed—even if it meant revealing metastatic disease. It’s frustrating because we know the cancer is somewhere and because we know the PSA almost tripled between 19 January 2024 and 16 January 2025, but we don’t have enough information to do anything about it. It’s just more waiting in limbo.
Of course, having had three PSMA PET scans all turn up negative makes me question if I’m in that “lucky” category of ten percent of patients whose prostate cancer doesn’t express PSMA, making the scans useless for me. It’s something that I’ll definitely discuss with the doctor at my next appointment on 1 April 2025. I vaguely recall that there’s some sort of genomic test that may be able to assess if I really do fall into that ten percent. I’ll have to do some research on that.
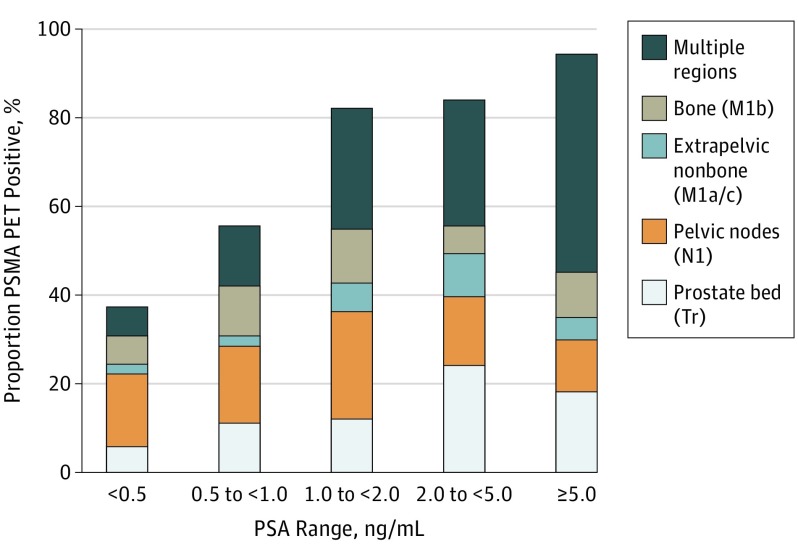
Maybe, too, I’ve placed too much faith in the scan’s ability to detect anything at my PSA level. But with a PSA level hovering around 1.0 ng/mL I thought we would have a decent chance of detecting something (chart below).
Detection Rate on a Patient Basis Stratified by PSA and Region Tr indicates prostate bed only; N1, pelvic nodes only; M1, extrapelvic only. Proportion of patients with 68Ga-PSMA-11 PET positive findings were stratified by PSA range and region of disease in accordance with PROMISE. https://pubmed.ncbi.nlm.nih.gov/30920593/
Needless to say, I’m truly glad that my PSA didn’t rocket even higher and that my scan didn’t light up like Times Square. Having definitive answers, though, would be the icing on the cake.
As far as the PSMA PET scan itself, it was pretty easy and took two hours to go through the entire process. I was instructed to drink 500 ml of water starting 2 hours before the scheduled scan time, and that was the only preparation needed.
I arrived at the hospital at 8 a.m. and was brought back to a radiation-proofed exam room where the technician started and IV at around 8:15 a.m. The 68Ga tracer was ready for injection around 8:40 a.m.
Around 9:30 a.m., the technician brought me back to the scanner where I got positioned on the bed and we began the scan which took 45 minutes. The scanner was very quiet (I could have dozed off) and large enough that it wasn’t claustrophobic. I was out of there by 10:15 a.m. and on my way home. Piece of cake.
On a related note, this was the longest it’s ever taken me to get the PSA test results posted online (hence the delay in this post). I actually called the clinic to get them over the phone because they still weren’t available online today (Thursday). The nurse I spoke with was very helpful and said, “We’re facing staffing issues and, well…” stopping herself in mid-sentence, probably remembering that the call was being recorded and not wanting to make a statement about the current environment for VA employees at the moment. I fear that this may be a precursor of things to come.
This will be a short update, as not much has really happened in the last month.
Tomorrow, I have my third PSMA PET scan. With luck, we’ll actually find the location of the cancer with this scan. That will help us decide what’s next in this adventure. I suspect I should be able to access the results online within a week or so. If not, I have a follow-up appointment on 1 April with the urologist.
I was going to get my PSA test done next week, but I wasn’t sure what impact a potential government shutdown might have on access to the lab, so I went for the blood draw on Monday. I’m guessing that I’ll break the 1.0 ng/mL threshold with this test.
That’s it for now. More to come in the days ahead.
Header image: Sunset over the Pacific Ocean, Silver Strand State Beach, California
Just as predicted, the scheduler took a couple of days to call. We’ve got the PSMA PET scan on the calendar for 12 March 2025, well ahead of the follow-up appointment with the urologist on 1 April 2025. No bone scan needed.