Late last week, I received a text message asking if I would like to move my urologist appointment from 30 December to today, 23 December, and I agreed.
My appointment was at 3:15 p.m., and I arrived around 2:45 p.m. As I’m walking up to the check-in kiosk, my cell phone rings, and it was the urology department wanting to confirm that I’d be there. That’s the first time that that’s happened, and I told the nurse that I was checking in as we spoke. “Great! We’ll come out and get you.” Apparently, they were antsy to get out of there early on the day before Christmas Eve. So was I.
The head of the department was the one who saw me this time, and we had a really good conversation. Some of the key takeaways:
- She was concerned about the increase in my PSA but not panicked, even initially suggesting we just continue to monitor it.
- We talked at length about doing another round of imaging to see if we can determine the location of the cancer.
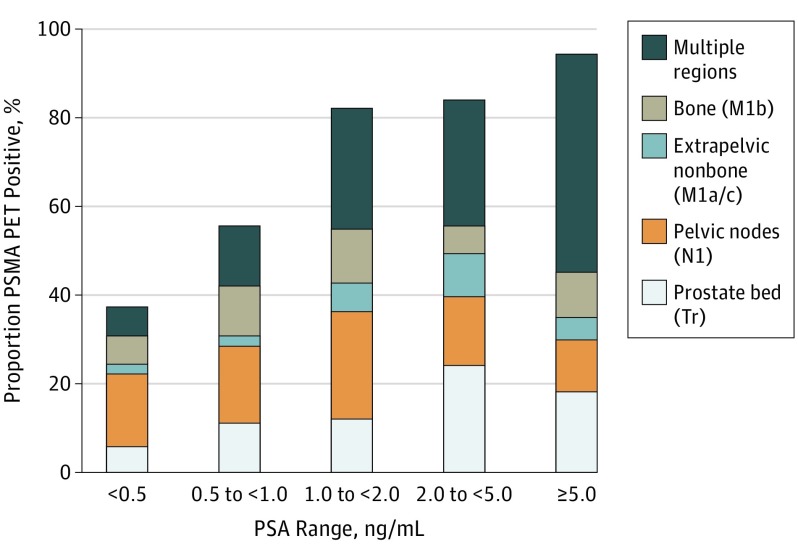
- We agreed to do another PSMA PET scan, and we negotiated doing one in March 2026. (She thought that Nuclear Medicine might push back on doing one sooner, i.e., within a year, as the last one I had was in March 2025.) She also mentioned the possibilities of other imaging should the PSMA PET scan come up with no evidence of cancer/metastasis for the fourth time.
- We talked about the timing of starting androgen deprivation (hormone) therapy. She wouldn’t start it until there was evidence of metastasis, but was open to starting it earlier if I really wanted to do so.
- Lastly, we reviewed my stress incontinence and nocturia issues and talked about my pelvic floor physical therapy.
It was one of the more thorough discussions that I’ve had at the VA, and I’m okay with the plan coming out of the meeting. I’ll go for another PSA test on 1 March; hopefully get the PSMA PET scan scheduled in early March; and have a follow-up with the urologist on 24 March.
I’m glad I got this out of the way before the holiday. I’ve got my answers, plus it frees up next week for me to go out an play if I want.
Merry Christmas, Happy New Year, and be well!
Header image: Hotel del Coronado at Christmas, Coronado, California