Well, that was a surprise at 3 p.m. on Good Friday afternoon.
A resident from the urology department called to let me know that she had reviewed my email with the original urologist and, after consulting with the nuclear medicine department, they came to the conclusion that I made a strong case for me getting an alternate scan.
Unfortunately, the VA doesn’t offer the Axumin scans, but they do offer Fludeoxyglucose F18 (FDG) PET scans which are also reliant on PSMA for the ligand to attach itself to.
She said that the F18 ligand interacts differently than the 68-gallium does, so it’s possible that it will attach to the PSMA molecules on the cancer cells. (In a prostate cancer forum, one patient was in a similar situation. The 68-gallium scans didn’t work for him, but a Pylarify PSMA PET scan did.)
I know from earlier reading that F18 FDG scans aren’t as sensitive and may not work best in a recurrent cancer situation, but they definitely won’t pick anything up if we don’t do them. She offered to put the order in to do one, and I said yes.
I’ll give nuclear medicine a few days next week to receive and process the order before calling them to schedule the scan.
I thanked the doctor at the end of the call and she, in turn, thanked me for advocating for myself.
I’ll post more when the date is scheduled, and I’ll be putting my list of questions together for the medical oncologist appointment on 14 April.
The scheduler called this afternoon and we set up an appointment with the medical oncologist (MO) on Tuesday, 14 April 2026.
Hopefully, I can enlist the MO as an ally in trying to get an alternate scan to see if we can find out what’s happening with the cancer.
I did write to the urologist on Monday to let him know that I came away from the phone call with a different understanding of what’s next compared to what he wrote in his summary notes. (My emails are included in my medical chart, and I wanted to be on the record that we had a disconnect in communications.)
I did my best to keep my emotion out of what I wrote, and tried to present it as me wanting him to further explain his viewpoint. I wrote, in part:
I agree with you that PSMA PET scans have become the gold standard for most patients. But we also know from multiple studies that 5% – 10% of patients don’t express PSMA and the scans won’t work for them.
I believe the fact that I’ve had four 68-Ga-PSMA-11 PET scans that haven’t located my cancer is strong, objective evidence that I may be in that small group of patients for whom the scans don’t work (barring any other possible test/proof that shows I don’t express PSMA). The last two scans should have had an 80% – 90% chance of detection at my respective PSA levels.
Please help me understand more definitively why you believe PSMA PET scans work for me, and what further evidence you would need to convince you that I may be in that group for whom the scans don’t work.
Finally, you stated that there was “limited likelihood that Axumin would provide additional clinically actionable information.” How would we know that unless we try? Axumin scans have an 80% chance of detecting something at PSA levels over 2.0 ng/mL.
We banked on PSMA PET scans to provide that clinically actionable information, yet time after time, they haven’t.
I’ll let you be the judge as to whether I kept the emotion out of my email. Again, the email to him went out Monday afternoon, so I wouldn’t expect a response for a few more days (if he’s even inclined to respond). I’m not sure if it was coincidence or if he pushed Oncology to call me because I did note at the end of my email that I hadn’t heard from them yet.
We’ll have to see how this plays out. More to come.
On the whole, the news is good. My PSA just barely bumped up from 0.94 ng/mL in January to 0.95 ng/mL in March and, taking the last five readings, that increased my PSA doubling time from 7.7 months to 10 months.
The PSMA PET scan revealed “no evidence of prostate cancer or metastatic disease.”
So, if the news is good, why am I “so over this?”
I was really hoping that this third PSMA PET scan would bring some clarity as to where the cancer was located so we could know how to proceed—even if it meant revealing metastatic disease. It’s frustrating because we know the cancer is somewhere and because we know the PSA almost tripled between 19 January 2024 and 16 January 2025, but we don’t have enough information to do anything about it. It’s just more waiting in limbo.
Of course, having had three PSMA PET scans all turn up negative makes me question if I’m in that “lucky” category of ten percent of patients whose prostate cancer doesn’t express PSMA, making the scans useless for me. It’s something that I’ll definitely discuss with the doctor at my next appointment on 1 April 2025. I vaguely recall that there’s some sort of genomic test that may be able to assess if I really do fall into that ten percent. I’ll have to do some research on that.
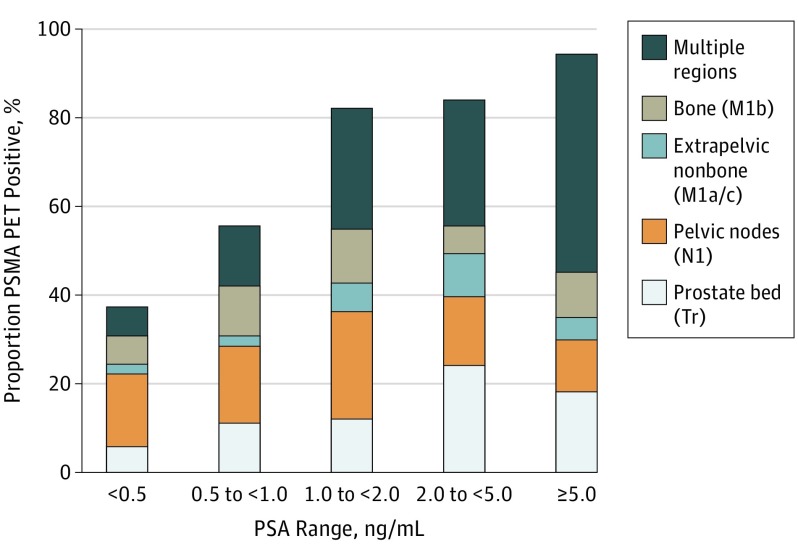
Maybe, too, I’ve placed too much faith in the scan’s ability to detect anything at my PSA level. But with a PSA level hovering around 1.0 ng/mL I thought we would have a decent chance of detecting something (chart below).
Detection Rate on a Patient Basis Stratified by PSA and Region Tr indicates prostate bed only; N1, pelvic nodes only; M1, extrapelvic only. Proportion of patients with 68Ga-PSMA-11 PET positive findings were stratified by PSA range and region of disease in accordance with PROMISE. https://pubmed.ncbi.nlm.nih.gov/30920593/
Needless to say, I’m truly glad that my PSA didn’t rocket even higher and that my scan didn’t light up like Times Square. Having definitive answers, though, would be the icing on the cake.
As far as the PSMA PET scan itself, it was pretty easy and took two hours to go through the entire process. I was instructed to drink 500 ml of water starting 2 hours before the scheduled scan time, and that was the only preparation needed.
I arrived at the hospital at 8 a.m. and was brought back to a radiation-proofed exam room where the technician started and IV at around 8:15 a.m. The 68Ga tracer was ready for injection around 8:40 a.m.
Around 9:30 a.m., the technician brought me back to the scanner where I got positioned on the bed and we began the scan which took 45 minutes. The scanner was very quiet (I could have dozed off) and large enough that it wasn’t claustrophobic. I was out of there by 10:15 a.m. and on my way home. Piece of cake.
On a related note, this was the longest it’s ever taken me to get the PSA test results posted online (hence the delay in this post). I actually called the clinic to get them over the phone because they still weren’t available online today (Thursday). The nurse I spoke with was very helpful and said, “We’re facing staffing issues and, well…” stopping herself in mid-sentence, probably remembering that the call was being recorded and not wanting to make a statement about the current environment for VA employees at the moment. I fear that this may be a precursor of things to come.
When you read the article, it omits any reference to gallium being used in medical diagnostics, so I have to wonder if this ban will adversely impact the ability to do 68Ga PSMA PET scans.
That question led me to a quick Google search on the production of 68Ga that yielded:
I’m no nuclear physicist or radiopharmaceutical guy but, given that process outlined above, it sounds to this layperson that PSMA PET scans could possibly be impacted.
Or I could be completely out to lunch, reading far too much into the story.
It’s definitely something to keep and eye on going forward, as I’m guessing another PSMA PET scan is in my future in January or February.
No evidence of recurrent prostate cancer or metastatic disease.
I know I should be excited but, at the same time, I don’t think I’ve been so frustrated by “good” news. Thanks to the steady increase in my PSA, we know something is happening somewhere, and I was really hoping this scan would end the game of cat-and-mouse that we’ve been playing trying to determine where the cancer is and what to do next. It didn’t.
Even though I recognized going into the scan that, at my PSA level (0.37 ng/mL), there was an approximate 40% chance of detecting something, I was hopeful it would come up with something this time. Silly me and my expectations.
Detection Rate on a Patient Basis Stratified by PSA and Region Tr indicates prostate bed only; N1, pelvic nodes only; M1, extrapelvic only. Proportion of patients with 68Ga-PSMA-11 PET positive findings were stratified by PSA range and region of disease in accordance with PROMISE. https://pubmed.ncbi.nlm.nih.gov/30920593/
The other thing I’m beginning to wonder is if I’m in that 10% of patients for whom PSMA PET scans don’t work. (You may recall that being mentioned in this video from the PCRI: Rising PSA After Prostatectomy.) I have to dig into that more to see if it’s just PSMA PET scans that use Gallium-68 as the tracer, or if that applies to any PSMA PET scan regardless of the tracer used. I’m guessing it’s the latter.
Choline and Axumin scans are another option, but they don’t start reliably picking up cancer locations until the PSA is at 1.0 ng/mL or higher. Assuming my current PSA doubling time (6.2 months) remains steady, that means waiting another 11 months before I hit 1.0 ng/mL for those scans to have a chance of seeing anything.
I’ll be putting together my list of questions for the urologist appointment on 13 February (I’m open to suggestions). I suspect we’ll have a good discussion on subsequent PSA testing, the value of knowing where the cancer is located at this point, and when to start hormone therapy.
Again, the silver lining in this is that my scan didn’t light up like the Las Vegas strip. I need to keep that in mind.
Again, going into this, I knew that there was a 50-50 shot that the PSMA PET scan would be able to pick up anything at my PSA level, and it appears that I fell into the “we didn’t see anything” category:
ONCOLOGIC FINDINGS:
History of prostate cancer status post prostatectomy with biochemical recurrence with: – No focal PSMA-uptake in the prostatectomy bed. – No PSMA-PET/CT evidence for distant metastasis.
The fact that they didn’t see anything in my prostate bed and elsewhere is both a good and bad thing. Good, in that whatever cancer may be there was so small that the scan couldn’t pick it up. Bad, in that the scan wasn’t sensitive enough to pick things up at my PSA level (0.22 ng/ml).
As a reminder, I’m just looking at the printout of my results online, and am not yet in a conversation with my doctor about the results, so I’m a little reluctant to come to too many conclusions about some other comments in the report without the benefit of his expertise. There was a section labeled:
INDETERMINATE FINDING:
– Focus of intense PSMA-uptake at the left lung lower lobe (fused 4-263) without CT correlate, likely a PSMA injection thrombus, not favored to represent metastatic disease. Attention on follow up.
I added the emphasis above, but it’s something that raises an eyebrow and probably warrants further monitoring or investigation as suggested. That’s something I’ll speak with the doctor about.
Speaking of speaking with the doctor, when I had my appointment in early November, we agreed to schedule a follow-up appointment to go over the scan results in January. However, the first available appointment wasn’t until the first week of February. I’m going to work on moving that earlier, even if it’s a call-in appointment instead of an in-person appointment.
Am I happy with the results? Sort of.
We know from my rising PSA that there’s cancer somewhere in some quantity. While this may be a “false negative,” it’s nice to know that I didn’t light up like the Rockefeller Center Christmas tree. That would have been bad.
Will this cause me to run to the radiation oncologist to start salvage radiation right away based on my PSA alone? Nope. I have another PSA test in January, and if that stays in the 0.21-0.22 range, I’ll be content to continue my monitoring. But if it shoots up drastically, that may cause me to reconsider.
Was it worth $3,300 out-of-pocket? I don’t know. I’m going to get back to you on that one. 🙂
So that’s my PSMA PET scan story, and I’m sticking to it.
If I don’t post again before Christmas, I hope you have a great holiday season!
As is often the case with medical tests, there’s a bunch of waiting involved. Even though the PSMA PET scan technician told me that the doctors would review the scan and have the results in 1-2 business days, apparently that didn’t mean that I’d have access to them right away.
After a week or so of hopping online, I emailed UCLA Nuclear Medicine to ask when I would be able to view the results on my online account. Their response:
Your results are set to auto-release in your account on 12/16/21 after 3:41pm.
Now that’s a rather specific date and time which seems quite unusual to me, but at least I have an answer. (It reminds me of my Navy days; see my sea story below.)
That would be my one complaint with UCLA. While the staff administering the scan was very patient-centric, the administrative end—not so much. I guess when you go to a world-renowned medical treatment facility, you’re just one of thousands and thousands of patients and personal attention becomes more challenging.
On a related note, I also alerted the VA San Diego to be on the lookout for the results and to contact me when they come in. So far, no luck.
More to come.
When I was a Surface Warfare Officer in the U.S. Navy, I qualified as Officer of the Deck, which meant that I stood watches on the bridge of the ship and was responsible for everything that went on during my 4-6 hour shift.
The captain of the ship (of all Navy ships) had something called Standing Night Orders for the Officers of the Deck to follow at night while the captain was asleep in his cabin. In the standing night orders, there was a place for the captain to write down whether or not he wanted a wake-up call and, if so, at what time.
On one of my first overnight watches with this captain, he put down that he wanted a wake-up call at 5:28 a.m.
That morning, I was busy with my head in the radar scope hood, trying to track and avoid colliding with another ship, and I missed the 5:28 a.m. call to the captain. But not to worry.
At 5:29 a.m., he was standing on the bridge in full uniform, brusquely asking, “Why didn’t you call me at 5:28 a.m.???”
Prick.
Fortunately, we had a change of command and received a new, human captain about 6 weeks later.
It’s over. The photos for my holiday cards are taken and ready to be processed. Look for a Christmas card with a cross section of my pelvis coming to you soon!
I had my 68Ga PSMA-11 PET and CT scans yesterday. In short, all went well but the technician couldn’t (or wouldn’t) tell me if the scan lit up like the Rockefeller Center Christmas tree. She said that images had to be processed first, and that she wasn’t trained to interpret them anyway. The doctors would have to do that in 1-2 business days.
The whole process took just under four hours—from the time I left my car in the parking garage to the time I got back in it.
The Process
Arrival
I checked into the Department of Nuclear Medicine about 40 minutes before my scheduled appointment (I was told 7 a.m. by the booking representative), and was told that my appointment was actually at 7:45 a.m. Oh well. It gave us a little time to complete the necessary paperwork and payment.
You’ll have several forms to complete, mostly asking about your current health status and history. Pretty easy. Just check the boxes and sign. You’ll also get one of those plastic wristbands with all of your information on it placed on your wrist. Mine initial band had my wrong birthday on it, so we had to have that corrected and a new wristband printed.
If you’re like me and your paying for it out of pocket, this is also where they’ll ask for your credit card (no cash or check) and charge the $3,300 fee.
Preparations
After you’re checked in, they’ll let the staff know that you’re there ready to begin the preparation process.
In the preparation room, the technician will insert an IV catheter into your arm that will be used to inject the 68Ga tracer and iodine contrast. As he does this, he’ll go through a very thorough explanation of what to expect once the scans begin.
He will also prepare another contrast that you take orally. It’s about 1 to 1.25 liters of a slightly yucky-tasting solution that you have to consume over the course of 45 minutes. They’ll also want you to reserve about 6 to 8 ounces of the fluid to gulp down just before you go in the scan. They want to have it in your stomach and not your intestinal tract. But you can’t start ingesting any of this until the 68Ga tracer is injected into your arm.
I believe that they actually manufacture the tracer on the spot for each patient. This is because, with its relatively short half-life, they can’t have it sitting around on a shelf waiting to be used.
When he returned with the 68Ga tracer, it was in this cute little container that I’m guessing was lead-lined to contain the radiation. He connected it to the IV catheter, juiced me up, and instructed me to start drinking the solution.
The last thing that he did was give me a little, “This guy is radioactive,” card to show to the authorities should I happen to set off sensors at airport or border security check points. Thankfully, I drove, so it wasn’t a concern for me.
That whole process took a little over an hour.
The Scans
Once you’re primed and ready to go, they’ll take you to the scanning room but they’ll ask you to stop by the toilet to empty your bladder first.
Interestingly the only articles of clothing that I had to remove were my shoes and jeans. Actually, they gave me the option of just pulling my jeans down below my knees or wearing a pair of hospital-provided pajama bottoms. I opted for comfort and the pajama bottoms.
They’ll place you on your back on the scanner bed and place a little cushion under your knees to make you feel a little more comfortable and, I suppose, to help better position you for the scan. You’ll raise both arms over your head and you’ll have to keep them there throughout the scan.
They’ll use your IV catheter to inject some iodine as a contrast. For me, the last time I had a CT scan and they injected the iodine, I became rather nauseated and told this technician about that incident.
She told me that they inject the contrast at a much slower rate than what’s used for a normal CT, and that should lessen the effects of the nausea. Even so, for insurance purposes, we put a little bib around my neck and a towel on my left shoulder just in case. “Try not to move your body if you do vomit.” Yeah, right. Good luck with that. Fortunately, she was right about the slower injection rate. The feeling was there briefly, but much less intense that before.
They’ll start with the PET scan first while the 68Ga tracer is still pretty strong, and it probably took about 25-35 minutes (I couldn’t see a clock for reference). Your only task is to stay completely still throughout. At the very beginning, you’ll be asked twice to inhale and hold your breath for about 10 seconds. After that, you just lay there, close your eyes, and enjoy the ride. (The scanning machine is nearly silent.)
Once the PET scan is done, they’ll send you off to the toilet once again to empty your bladder before the CT scan.
You’ll get back in position onto the scanner bed just as before—knees propped up and arms above the head—and they’ll begin the CT scan. The technician said it would take 8 minutes, but it seemed closer to 15 minutes to me.
When you’re done with the CT scan, you’re done. You get dressed and head home—I didn’t have to stop at the reception desk afterwards. They will tell you, however, to drink lots of fluids (preferably water) to flush the contrasts from your system.
They will forward the results to the physician who ordered the scan.
Effects
Aside from a slight metallic taste in my mouth and being really hungry after fasting in advance of the scans, I felt fine leaving the hospital. My shoulders were a little sore from holding my arms above my head for an hour or so, and that was about it.
When I arrived home, though, it all caught up with me. I was spent.
During the whole process, I felt very calm and relaxed, so I didn’t think it was stress-related fatigue, but I guess our subconscious can play games with us. It may have had something to do with waking up at 4 a.m. and not being able to fall back asleep, too. Or a combination of all of the above. Regardless, I just crashed on the sofa and took a nap.
One other thing that happened yesterday afternoon was that I had a bunch of gremlins doing a jig in my stomach that caused me to run to the toilet half a dozen or so times. (TMI, I know.) Whether it was related to the contrasts or the hot giardiniera peppers I had on my Italian beef sandwich at lunch, I don’t know. Needless to say, it wasn’t anticipated either way. I’m better this morning, with a few lingering grumbles going on down there.
Logistics
Scheduling
Regular readers already know the hassle I went through trying to get San Diego VA Medical Center to talk with UCLA Department of Nuclear Medicine, so I won’t rehash that here. Needless to say, be persistent if you encounter similar issues.
I did find it interesting that the scheduler told me my appointment was at 7 a.m. when it was actually at 7:45 a.m. I’m not sure how or where that disconnect came into play.
Lodging
Because my appointment was so early in the morning, I opted to drive from San Diego to Los Angeles the afternoon before and stay in a nearby hotel to the tune of $216. Apparently, UCLA has its own hotel at the convention center, but the price would be about the same, if not more.
Location
Obviously, UCLA is a huge campus and I wished that the scheduling office provided more information about where the building was, where to park, and where the Nuclear Medicine department was located when they set the appointment. They provided nothing until I asked.
They are located at 200 Medical Plaza Driveway Suite B114, Los Angeles, CA 90095.
When you pull in from Westwood Blvd. to Medical Plaza Driveway, you’ll turn right but will want to be in the left lane to enter the parking garage (red arrows below).
Entrance to parking garage from Westwood Blvd (red line) and walk inside the building from the lobby to the North Elevators (blue line).Photo from Google Maps.Entrance to parking garage (red arrow) and walk along the front of the building (inside) from the lobby to the North Elevators.Photo from Google Maps.
Once you’re in the parking garage, you can take the elevators on the west side of the building up to the lobby. You’ll walk all the way across the lobby and follow the signs for the North Elevators (blue line above). Take the North Elevators down to Level B1 and the Nuclear Medicine department is right off the elevators in Suite B114.
Parking is $14 per day and, no, they won’t validate your parking ticket even after spending $3,300.
Final Thoughts
First, the staff in the Nuclear Medicine department were amazingly friendly and caring. It made the whole experience all that much better.
Second, I’ll have to admit that I second-guessed myself in wanting to have to get this done after the insurance company denied the payment. Not because of the cost (although it’s not insignificant), but because I knew from my own research that the 68Ga PSMA-11 PET scans are better at picking up the location of the cancer when the PSA level is 1.0 ng/ml (the insurance company threshold), than at my 0.22 ng/ml PSA level. Am I wasting $3,300 on a crap shoot? We’ll soon find out.
Finally, there’s the, “If you can’t stand the answer, don’t ask the question,” factor in play here. If the scan wasn’t a crap shoot and does, in fact, reveal the location of the cancer, the pressure to act (i.e., salvage radiation) goes up by an order of magnitude. As you already know, I’ve been trying to dodge the short and long-term toxicities of salvage radiation for quite some time now, and my preference would be to continue to do that for as long as I can. There will be more research and decisions in the days and weeks ahead, that’s for certain.
Let’s just hope that getting the results from UCLA to VA San Diego won’t be as difficult as getting them to talk to each other in the first place.
Over the weekend, I received a letter from my health insurance company explaining the denial of covering the cost of the PSMA PET scan. This differs from what the representative told me via email (UCLA didn’t send all of the necessary paperwork) and carries far more weight, as it appears that a medical review was done. The redacted section below is the name of my insurance provider.
In a nutshell, because my PSA is 0.22 ng/ml, it doesn’t reach their threshold of 1.0 ng/ml, they deem the scan “not medically necessary” and won’t cover the cost.
The insurance company may have a limited point in their comment, “Use of this study would [not] improve the outcome” with my PSA level being so low. Realistically, the chances of the cancer metastasizing while waiting for the PSA to go from 0.22 to 1.0 are miniscule—especially with my PSA doubling time—and the treatment options would likely be the same: Salvage radiation, perhaps with hormone therapy as well.
However, the insurance company is missing the larger point: The whole purpose of having highly sensitive, highly specific scans like 68-Ga PSMA PET is to locate cancer early so that you can come up with an effective treatment plan that hopefully does, in fact, have a positive impact on the outcome and survival.
My urologists were supportive of getting the scan, so I’ll see if I can’t get them to help convince my insurance company through a formal appeal that this is, in fact, medically necessary.
As far as the scan itself, it’s less than 24 hours away. UCLA Department of Nuclear Medicine did remind me that I have to fast for at least six hours prior to the scan, drinking only water. No juice, no coffee, just water.
On Tuesday, UCLA called to confirm my PSMA PET scan next week and, during the call, the said that they had not yet heard from my health insurance company as to whether or not they would cover the cost of the scan. She asked if I wanted to proceed next week, paying the $3,300 myself, or delay until the insurance was settled. If I delayed, the next available appointment would be in February 2022.
I told her to keep next week’s appointment and that I would battle it out with the insurance company after the fact.
On Wednesday, UCLA calls saying that my insurance had denied the request for the scan and wouldn’t cover the cost. Again, I reiterated that I would keep the appointment and pay the cost myself.
But I was curious about the reason for my denial, as I had an email from my health insurance company earlier in the year indicating the values that they would pay for each of the CPT codes that were given for the scan, so I emailed them again (after trying to get through on the phone on the day before Thanksgiving failed).
I was actually surprised that I received a response this morning that read:
I accessed your account and I see that the pre-approval was denied because of insufficient medical records was [sic] provided from the provider. I request you to please ask the provider to call…and verify the documents needed to submit for prior authorization then send the documents so that we can approve it.
Of course, UCLA is closed for the holiday weekend today, and I’ll have to just try to get them to get this taken care of on Monday when I go up there.