The scheduler called this afternoon and we set up an appointment with the medical oncologist (MO) on Tuesday, 14 April 2026.
Hopefully, I can enlist the MO as an ally in trying to get an alternate scan to see if we can find out what’s happening with the cancer.
I did write to the urologist on Monday to let him know that I came away from the phone call with a different understanding of what’s next compared to what he wrote in his summary notes. (My emails are included in my medical chart, and I wanted to be on the record that we had a disconnect in communications.)
I did my best to keep my emotion out of what I wrote, and tried to present it as me wanting him to further explain his viewpoint. I wrote, in part:
I agree with you that PSMA PET scans have become the gold standard for most patients. But we also know from multiple studies that 5% – 10% of patients don’t express PSMA and the scans won’t work for them.
I believe the fact that I’ve had four 68-Ga-PSMA-11 PET scans that haven’t located my cancer is strong, objective evidence that I may be in that small group of patients for whom the scans don’t work (barring any other possible test/proof that shows I don’t express PSMA). The last two scans should have had an 80% – 90% chance of detection at my respective PSA levels.
Please help me understand more definitively why you believe PSMA PET scans work for me, and what further evidence you would need to convince you that I may be in that group for whom the scans don’t work.
Finally, you stated that there was “limited likelihood that Axumin would provide additional clinically actionable information.” How would we know that unless we try? Axumin scans have an 80% chance of detecting something at PSA levels over 2.0 ng/mL.
We banked on PSMA PET scans to provide that clinically actionable information, yet time after time, they haven’t.
I’ll let you be the judge as to whether I kept the emotion out of my email. Again, the email to him went out Monday afternoon, so I wouldn’t expect a response for a few more days (if he’s even inclined to respond). I’m not sure if it was coincidence or if he pushed Oncology to call me because I did note at the end of my email that I hadn’t heard from them yet.
We’ll have to see how this plays out. More to come.
Those of us of a certain age may remember the “Stump the Band” segment on the Johnny Carson show, where audience members asked the band to play some obscure song. Well, today was my turn at “Stump the Urologist.”
It was a very productive meeting that lasted nearly 40 minutes which was unusual. I came equipped with hard copies of my PSA chart, the MSKCC PSA doubling time (PSA-DT) calculator results, and my list of questions. He was impressed and really pleased with the chart in particular.
We started talking about how my four PSMA PET scans were all inconclusive, and I steered the conversation to whether I might be one of the 10% for whom PSMA PET scans don’t work. He seemed to be a bit skeptical at first, but he also said it was a possibility.
Given that my PSA increased substantially and my PSA-DT was decreasing, I wondered if it would be better to jump into ADT sooner or if there’s still value in trying to find the cancer’s location with imaging. He was of the opinion to continue to try to find it before starting ADT.
I had a series of questions that really dealt specifically with ADT, and he said it was a bit premature to think about those and that they would be better answered by a medical oncologist. I knew that I was jumping the gun with some of them, but I thought I’d ask anyway. During that part of the conversation, I did mention that I tolerated the ADT probably better than most when I had it for my salvage radiation therapy, but that I wasn’t eager to jump into it earlier than necessary.
After that, he took control of the conversation and asked me about my status when it came to sexual function and incontinence, and offered up options to deal with both if I was interested.
Then we returned to the topic of next steps, and that’s where I played “Stump the Urologist.” (Who, by the way, was a full-blown internist and not a resident.) He grabbed my PSA chart and excused himself for a few minutes as he went off to consult with the department head.
When he returned, I was a bit surprised when he put his faith in the results of the PSMA PET scan, saying it has the best sensitivity and the best specificity of any scan out there. He said that they had moved away from the Axumin scans because they were the old technology.
I politely pushed back, reminding him that a PSMA PET scan should have had an 80% – 90% chance of finding my cancer at my PSA level if I had the PSMA protein for the 68-Gallium tracer to lock onto. But if I don’t have that PSMA protein, the sensitivity and specificity of the scan won’t matter because nothing will ever light up. He really couldn’t argue against that.
I went back to the topic of ADT and mentioned that I met with a medical oncologist (MO) two years ago, and received conflicting opinions on when to start ADT. The MO said she would start my ADT when my PSA hit 2.0 ng/mL (a urologist said she wouldn’t start it until there was evidence of metastasis). Today’s urologist said he looks for one of three “triggers” to begin ADT: PSA > 10.0 ng/mL 😲; PSA-DT less than six months; or evidence of metastasis.
I also mentioned that the VA MO that I saw two years ago was a general oncologist and not someone who specialized in genitourinary cancers and, as helpful as she was, she had to consult with a UCSD MO who specifically deals with prostate cancer. I sowed the seed of eliminating the VA MO as a middleman if they have to consistently consult the UCSD doctor (who is highly regarded in the field), and suggested that I could just see him directly. I’m not sure if that will take root.
Finally, I did ask a very basic question given how elusive this has been: Is this even cancer? He said that, if I hadn’t had a prostatectomy, that there might be other explanations for the rising PSA. But he was confident that we are, in fact, dealing with cancer.
That led to a follow-up question of: Is it metastatic? Based on the information we have, he said it’s not. He seemed to squirm a bit when I asked about it being micro-metastatic, because, in his mind, that wasn’t very well-defined.
Before mapping out a plan, I have to admit that my ego puffed up a tad when he said, “You’re the best educated patient I’ve seen in weeks.” He also admitted that my case was a bit puzzling to them and not something they routinely see.
We agreed on three actions:
The doctor is going to explore how and where I can get an Axumin scan, and if the VA will authorize it if I have to go outside the VA. That may take a day or two to get an answer. I mentioned that I’d be willing to use Medicare and go out on my own if necessary.
He is doing a referral to get me seen by the VA oncology team to get them familiar with my case. I suspect it will take a few days to hear from the scheduler.
We do another PSA test in June and meet to see where we’re at.
All in all, this was a good meeting with a robust discussion about my case that has all of us scratching our heads as to what’s going on and what to do next. Frustrating? Yes, to a degree. But, as we discussed during the meeting, nothing is black-and-white in the world of prostate cancer.
More to come.
Be well!
For my readers outside the U.S. who may not be familiar with Johnny Carson, I was going to link a random video clip of his “Stump the Band” segment above and, when I searched YouTube, this—of all clips—was the one that popped up first. I think you’ll see the related humor in it once you watch it. 😂
Header image:Anza-Borrego Desert State Park, California
My visit to the urologist this afternoon went just as expected, and even a little better.
With the San Diego VA Medical Center being a teaching hospital, it’s rare that I see the same doctor twice. Because I liked the doctor I saw last time because of the conversation we had and the plan that we mapped out together, I specifically requested to see her again this time. Unfortunately, a young resident showed up in her place.
That actually may have worked to my advantage.
Dr. K started the conversation by asking if I had come to a decision as to whether I wanted to do salvage radiation therapy or hormone therapy. I was a bit taken aback by that—”Haven’t we skipped a few steps here, Doc?”—but then I remembered the way that Dr. L wrote up her notes from my visit with her, it would be easy for him to come to that conclusion.
I filled in a few of the blanks with Dr. K regarding our plan to follow up the negative CT and bone scans with an Axumin or PSMA PET scan in hopes of finding the cancer before making the SRT vs. ADT decision. He dutifully reminded me that either or both scans could come back negative, too, meaning that the cancer was still likely in the pelvis or prostate bed.
Interestingly, when we were talking about the merits of the Axumin and PSMA PET scans, he immediately went to, “Why even bother with the Axumin scan; go straight to the PSMA scan.” I didn’t even have to nudge him in that direction. He and I were on the same page.
To his knowledge, though, SD VAMC had not yet referred anyone to get a PSMA PET scan, but he seemed eager to figure our how to make it happen and have me be the first (or among the first) to be referred. He wasn’t even sure where to begin, so I told him.
Instructions for PSMA Referral
I opened my file folder that I had with me and pulled out the one-page sheet that I had put together, stepping him through the referral process that UCLA had shared with me. It was all there for him, and he asked, “May I keep this?”
He did admit, though, that he had no idea how long it may take to get approval from the hospital team before he could even ask for the referral, so this may play out over a few weeks or longer. Rest assured that I’ll keep on top of this, asking for periodic updates.
I’m pretty excited that we’re moving in the direction of going straight to the PSMA PET scan, but also recognize there can be a number of administrative twists and turns along the way.
In the interim, we agreed to test my PSA again in early November, keeping on a four-month testing cycle. I’m okay with that while we’re trying to sort everything else out.
We also talked about my incontinence episodes becoming more frequent and more substantial in the last 6 weeks or so. He wanted to rule out a urinary tract infection, so he sent me off for some labs and we’ll see what they yield.
These episodes have put me back in incontinence pads for the last few weeks. Before, a sneeze or a cough would yield a few drops; now, they yield a squirt. Not good.
As a baby boomer, I grew up with Spock. Both of them.
First, there was Dr. Benjamin Spock, the noted pediatrician who told my parents—and millions of other parents—how to raise and care for their kids. Then, of course, there was the Star Trek Spock, whose existence was rooted in Vulcan logic.
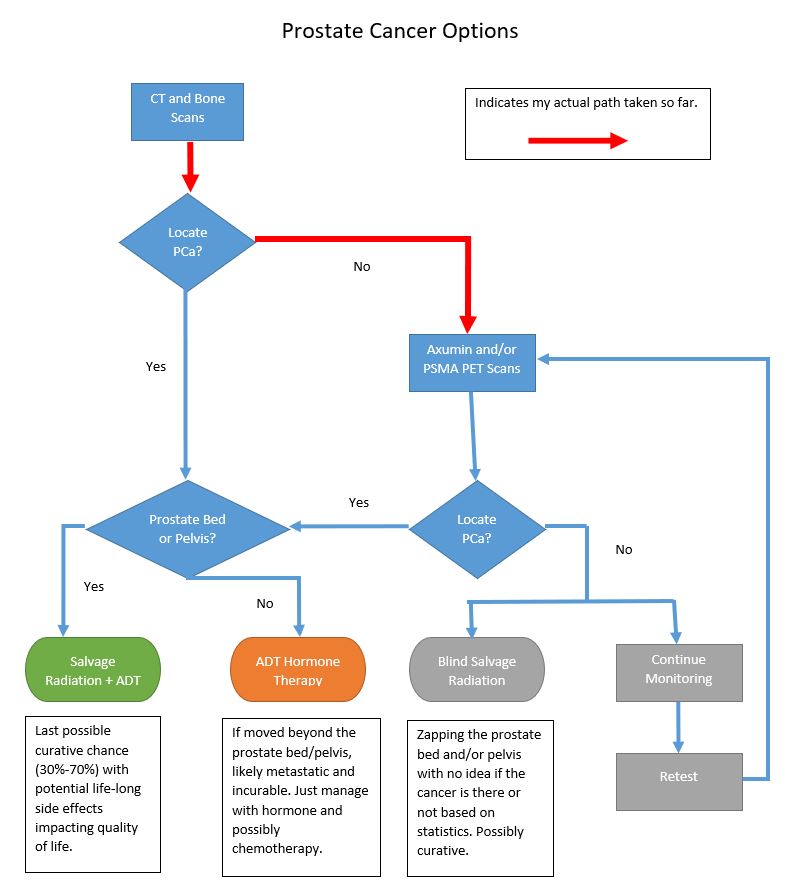
Now I’m not a Trekkie, but if you’ve read any part of this blog, you do know that facts, figures, and logic are high on my priority list, too. I thought, “What better way is there to outline the possible scenarios and decisions that are ahead of me than to put them all in a flow chart.” So here goes:
So let’s step through this.
We start with the CT and Bone scans that happened over the last two weeks. The first question is, “Did those scans determine the location of the prostate cancer (PCa)?”
If the answer is yes, then the next question is, “Was the prostate cancer in the prostate bed and/or pelvis?”
PCa in Prostate Bed/Pelvis
If the answer is yes, the PCa is in the prostate bed and/or pelvis, then Salvage Radiation Therapy (SRT) with or without Androgen Deprivation Therapy (ADT) (Hormone therapy) offers the last possible chance of a true cure. Of course, there are risks associated with SRT that would impact your daily quality of life: bowel control, bladder control, and lack of sexual function. Additionally, depending on which study you look at, SRT may be successful only 30% to 70% of the time. (Green bubble above.)
PCa is Not in Prostate Bed/Pelvis
But if the answer is no, the PCa is outside of the prostate bed and pelvis, that means the PCa is now distant and likely metastasized. If that’s the case, there is no cure and the PCa can only be managed with hormone therapy and perhaps chemotherapy. (Orange bubble above.)
CT and Bone Scans do not Locate the Prostate Cancer
We’ve talked at some length that neither the CT scan nor the bone scan have the sensitivity to pick up the cancer’s location based on my PSA level of 0.21 ng/mL. It was very likely that neither would pick up the cancer at that first decision point on the flow chart, so further investigation is required by using the Axumin or PSMA PET scan.
CT and Bone Scan Results
In fact, neither the CT nor the bone scan picked up the location of the cancer:
No definite scintigraphic evidence of metastatic bone disease and no evidence of a widespread osseous process
So that’s actually good news with the bone scan. It shows that it has not metastasized to the bones, which is definitely a good thing. (Or, at least if there is metastasis to the bones, it’s at a level that’s unable to be picked up by the sensitivity of the scan.)
Next Steps
We follow my red arrows above and run the Axumin or PSMA PET scans (or both) to see if either of those can pick up the location of the cancer. I’ll have that discussion with the urologist on 3 August 2021, and we’ll see when we can get them on the calendar.
If the Axumin and/or PSMA find the cancer in the prostate bed/pelvis, then we go back to the section above and land on SRT as the option. But if it’s found outside the prostate bed/pelvis, then we go back to the other section where we just manage with ADT. (If the lesion outside the pelvis is well-defined, it may be something that could be zapped in its location. Something to explore.)
If the Axumin or PSMA PET scan cannot locate the PCa, then things get fuzzy fast.
Sure, we could go ahead and blindly complete the salvage radiation therapy, hoping that we’re zapping in the correct place. Or, we could continue to monitor for a while longer and then retest to see if the cancer can be pinpointed.
This may have been a bit of an oversimplification of what’s ahead for me, but I’m hoping that it makes sense to you.