The short version from yesterday’s appointment with the urologist (who happens to be the Urology Department head):
Kick the proverbial can(cer) six months down the road and retest PSA then.
Generally speaking, I’m okay with that approach. I mean, really, what else is there to do at this point? We don’t have sufficient data points to make any definitive treatment decisions right now. Of course, I may feel differently after sleeping on this for a few nights.
I have to admit that it was a challenging meeting because the doctor just wanted to rapid-fire through all the discussion points and it was difficult to get my questions out. In the end, though, I prevailed.
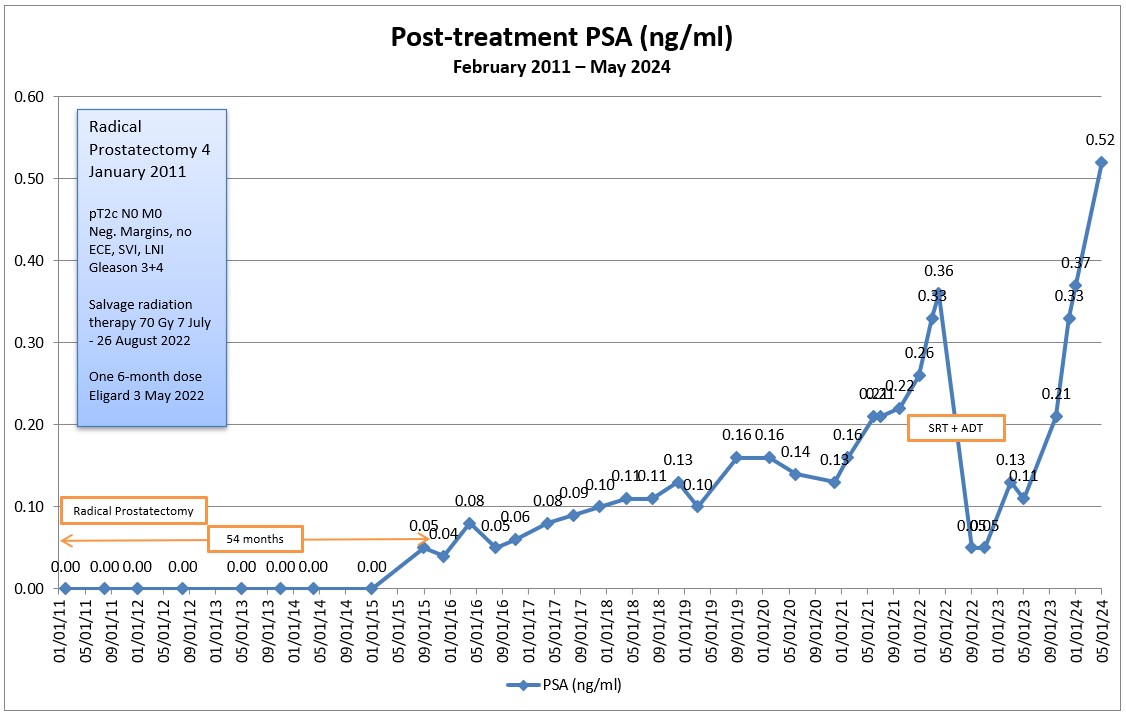
She was blasé about the increase in my PSA, saying it went up “a little bit.” (A 41% increase in my mind is a tad beyond “a little bit,” but what do I know?) She didn’t see much value in doing another PSMA PET scan right now because a scan with a PSA of 0.52 ng/mL has about a 50-50 chance of detecting anything. That somewhat aligns with what the medical oncologist (MO) said in February—that it would be better to wait until my PSA was at least 0.7 or 0.8 before doing another scan.
My SWAG (scientific wild-assed guess) is that my PSA will be between 0.75 ng/mL and 1.1 ng/mL in November based on the average increases in my PSA over the last four readings and my PSA doubling time. (Bookmark this prediction for future reference! 😀)
We did talk about androgen deprivation therapy. Her biggest concern was that starting too early would just accelerate the eventual likelihood of resistance later on when ADT is needed the most, so she wouldn’t start ADT until there’s confirmed metastasis. (By comparison, the MO suggested holding off until my PSA hit 2.0 ng/mL.) I did ask if starting ADT early delays metastasis and she said it didn’t, which I thought was interesting.
We talked about whether it would be a monotherapy or a combination therapy, and she suspected we would start with just a monotherapy. She acknowledged that there are several studies out there showing that a combination therapy may lead to better outcomes but, in her mind, they weren’t persuasive enough to launch straight into combination therapy. However, she did say that there are certain circumstances where it may make sense, one of which was if the metastases was in the spine.
I asked about possible radiation of localized lesions and she was not all that enthusiastic about the idea. Her biggest concern was about going through radiation twice and whether that was a wise thing given what damage it may do to my body. “I’d have to defer to the radiation oncologist to make that assessment,” she said. Her fear was additional radiation damage / side effects, and I would have that same concern, too. I would have to consider very carefully zapping anywhere in the pelvic area again given the changes I have already experienced in my bowel habits.
Even if the scan showed one or two lesions that could be zapped, she would also start ADT because “it’s pretty much guaranteed that there would be cancer elsewhere that didn’t light up on the scan.” That makes sense.
Lastly, given where I’m at in this advanced prostate cancer no-man’s land, I was curious how she would label or stage my cancer. With no evidence of metastases on the last scan, she would still have me at Stage 2. (See the American Cancer Society staging of prostate cancer HERE.)
Of course, in my mind, I turned to the actual definition of metastasis:
the spread of a disease-producing agency (such as cancer cells) from the initial or primary site of disease to another part of the body
I don’t have a prostate (initial or primary site) but I do have evidence of cancer, so it must be in “another part of the body.” By that definition, it must mean that I’m metastatic, right? (Yeah, I know… Nothing in the prostate cancer world is that clear.)
I asked the question about staging more as an academic exercise because it really doesn’t matter much what the label or stage is. All I know is that I’m living with this bug growing inside me.
One of my blog followers, Phil, recently commented that his oncologist considered prostate cancer to be more of a chronic illness than a terminal illness, and that stuck with me. I mentioned that to the doctor, and she embraced that view wholeheartedly, telling me that patients like me can be kept around for many years—even decades—and the disease can be managed like hypertension or diabetes.
Intellectually, I already knew that. But, after 13+ years, it’s quite the mental leap to jump from, “I have the Big C and it continues to grow unabated,” to, “Cancer, schmancer. It’s like arthritis in my big toe. No big deal.” But it is a leap I’m trying to make.
You would expect that, after 13+ years of testing, waiting for results, reviewing results, and planning next steps, I’d be used to it by now. It’s routine. But I’m finding it to be more and more emotionally draining with each cycle as the uncertainty drags on. Perhaps it’s because I’m coming to terms with failed treatments when I had hopes for better outcomes, or perhaps it’s because I’m back in the wait-and-see mode. Or maybe it’s just the cumulative effect of being on this roller coaster for so long.
On the positive side, I know that I’ve been blessed. Many fellow prostate cancer patients would love to have their PSAs be at my level; my quality of life is pretty good considering all that my body has been through; and—most important—I’m still here 13+ years after diagnosis.
On a somewhat related note, I finally got my baseline testosterone results back: 424 ng/dL. That was taken almost two years to the day after receiving my six-month Eligard shot in advance of salvage radiation therapy, so I’m guessing that any effect the Eligard may have had on my testosterone level has worn off by now.
From what I can tell, that’s a decent / normal number for a 66-year-old guy.
At least we have a starting point for reference now.
Well, that’s it for this post. Time to go out and play for six months. Be well!
What’s next:
- Week of 28 October – Get PSA test
- 4 November – Physical with primary care physician
- 14 November – Appointment with urologist
Header Image: La Jolla Coast, San Diego, California